BIASES – EXAMPLES IN THE 2016 NHMRC DRAFT REPORT
Fluoride destroys 66 of the 83 known enzymes
and is thus a blocker to re-enamelization.
~ The Obsolete Practice of Water Fluoridation ~

Last update: 17 Feb. 2020
This section of our site will provide information on how to grow good teeth
and how to care for them. Please revisit this post as we shall be
adding more information in the near future.
THANK YOU
→ Fusobacterium nucleatum ←
→ International Academy of Oral Medicine & Toxicology ←
![]()
‘CURE TOOTH DECAY’
by
Ramiel Nagel
Extract→ HERE ←
![]()
FLUORIDE DESTROYS ENZYMES:
The re-enamelization (remineralization) of tooth enamel requires the enzyme adenosine diphosphatase, as well as supplemental calcium and phosphate in the diet. Furthermore, remineralization of the dentine underneath the enamel requires calcium, phosphate and adenosine diphosphatase. Dentine has been shown to repair also, even after the onset of bacterial attack. Be aware, though, that re-enamelization (remineralization) cannot occur without adenosine diphsphatase and perhaps other enzymes. Fluoride destroys 66 of the 83 known enzymes and is thus a blocker to re-enamelization.
(Cholinesterase is compromised at .0095 ppm and Calcium adenosine diphosphatase at .00037 ppm of fluoride.)
→ → → CLICK HERE ← ← ←
PROFESSIONAL PERSPECTIVES U-TUBE

See extracts below ↓ ↓ ↓

.
Recommended Reading
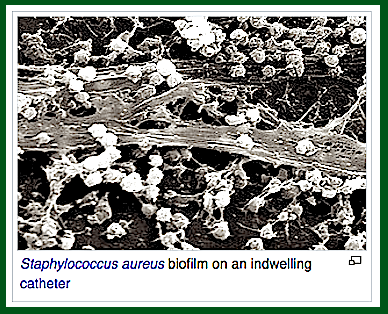
→ BIOFILMS ←
“…Biofilms can attach to a surface such as a tooth, or rock, and may include a single species or a diverse group of microorganisms. The biofilm bacteria can share nutrients and are sheltered from harmful factors in the environment, such as desiccation, antibiotics, and a host body’s immune system…”Biofilms can form on the teeth of most animals as dental plaque, where they may cause tooth decay and gum disease.
[ MMS (a) – MMS (b) – MMS (c) will control biofilms]
. ![]()

MOREExtract from:
Investigation of Defluoridation Options for
Rural And Remote Communities
Amy Dysart Power Water Corporation
Research Report No. 41
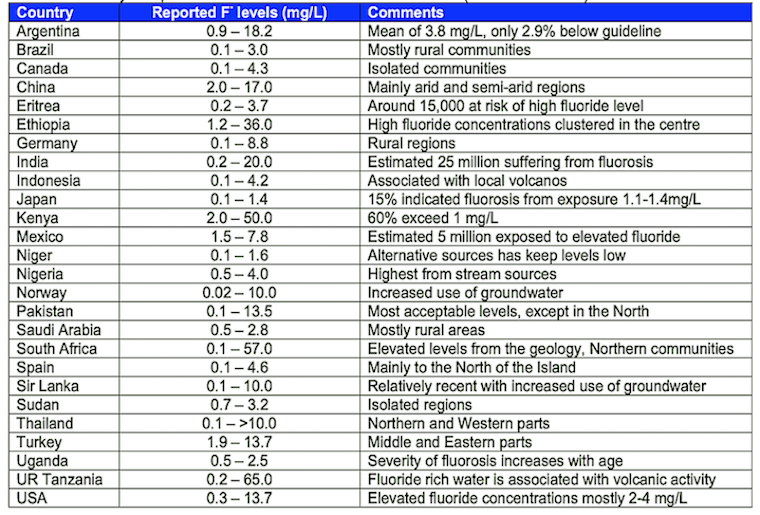
Groundwaters with high fluoride concentrations occur in many areas of
the world including parts os Africa, China, the Eastern Mediterranean
and Southern Asia ( India, Sri Lanka) and is a serious problem in
developing countries (Table 4). Generally, in the USA and in
Central Europe, The fluoride concentration of natural water
is at the lower end of the range (Fletcher and Smith 2003).
Table 4. Summary of reported fluoride levels in a
number countries (Fawell et al. 2006)
Queensland Towns No Longer Fluoridated – July 2018
A need for Better Evaluation of fluoridation.
FLUORIDATION SURVEYS IN AUSTRALIA
The “tooth patch” is a hard-wearing and ultra-flexible material made from hydroxyapatite, the main mineral in tooth enamel, that could also mean an end to sensitive teeth.
“This is the world’s first flexible apatite sheet, which we hope to use to protect teeth or repair damaged enamel,” said Shigeki Hontsu, professor at Kinki University’s Faculty of Biology-Oriented Science and Technology in western Japan.
“Dentists used to think an all-apatite sheet was just a dream, but we are aiming to create artificial enamel,” the outermost layer of a tooth, he said earlier this month.
Researchers can create film just 0.004 millimetres (0.00016 inches) thick by firing lasers at compressed blocks of hydroxyapatite in a vacuum to make individual particles pop out.
These particles fall onto a block of salt which is heated to crystallise them, before the salt stand is dissolved in water.
The film is scooped up onto filter paper and dried, after which it is robust enough to be picked up by a pair of tweezers.
“The moment you put it on a tooth surface, it becomes invisible. You can barely see it if you examine it under a light,” Hontsu told AFP by telephone.
The sheet has a number of minute holes that allow liquid and air to escape from underneath to prevent their forming bubbles when it is applied onto a tooth.
One problem is that it takes almost one day for the film to adhere firmly to the tooth’s surface, said Hontsu.
The film is currently transparent but it is possible to make it white for use in cosmetic dentistry.
Researchers are experimenting on disused human teeth at the moment but the team will soon move to tests with animals, Hontsu said, adding he was also trying it on his own teeth.
Five years or more would be needed before the film could be used in practical dental treatment such as covering exposed dentin — the sensitive layer underneath enamel — but it could be used cosmetically within three years, Hontsu said.
The technology, which has been jointly developed with Kazushi Yoshikawa, associate professor at Osaka Dental University, is patented in Japan and South Korea and applications are under way in the United States, Europe and China.


From ‘Keep 32′ [teeth]
No more fillings as dentists reveal new tooth decay treatment ↓
New info → HERE ← Jan. 2015
↓ SEE NEW INFO BELOW ↓
Keep 32 molecule discovered, kills the bacteria that causes tooth decay
→ HISTORY OF FLUORIDATION IN CAVITY PREVENTION ←
❝ The sign of fluoride over-dose [dental fluorosis] is now pandemic in fluoridated areas.
The teeth are a mirror of what also occurs in our bones. ❞
In contrast to skeletal bone and dentine, which accumulate fluoride throughout life and in proportion to the absorbed dose of fluoride, enamel of teeth reflects the biologically available fluoride at the time of tooth formation. Enamel maturation of deciduous teeth is completed between the age of 2 to 12 months. In permanent teeth enamel maturation is completed at the age of 7-8 years, except in the third molars, in which it continues until the age of 12-16 years. Post-eruptive fluoride uptake of enamel is expressed only in the outer layer and depends on fluoride in saliva, food, dental plaque and dental products (WHO, 1994). In areas with low fluoride concentrations in drinking water (≤0.1 mg/L) the fluoride concentration at 2 micrometer depth of enamel averages 1700 mg/kg, with fluoride concentrations in water of 1 mg/L it is 2200-3200 mg/kg. When water contains 5-7 mg/L of fluoride the concentration in enamel has been 4800 mg/kg. Such concentrations usually are accompanied by dental fluorosis (NRC, 1993).
About.com Guide Updated 15 December 2003
About.com Health’s Disease and Condition content is reviewed by our Medical Review Board
Wednesday January 24, 2001 ––Cavity rates declined in several cities that stopped water fluoridation, new studies report, contradicting American Dental Association (ADA) predictions, according to Fluoride Action Network.
Fluoride added to over 62% of US water supplies is supposed to reduce tooth decay, but these six studies from dental journals show it hasn’t and, in fact, may have increased the likelihood of rotten choppers. “No increase in caries (cavities) was found in Kuopio (Finland) 3 years after the discontinuation of water fluoridation,” according to Caries Research
(1).
In fact, when Kuopio was compared to a similar never fluoridated Finnish town, cavity rates in both towns either remained the same or decreased six years after fluoridation was stopped in Kuopio.
Seven years after fluoridation ended in La Salud, Cuba, cavities remained low in 6 to 9 year olds, decreased in 10 to 11 year-olds, significantly decreased in 12 to 13 year olds, while caries-free children increased dramatically, reports Caries Research
(2).
East German scientists report, “following the cessation of water fluoridation in the cities Chemnitz (formerly Karl-Marx-Stadt) and Plauen, a significant fall in caries prevalence was observed,” according to Community Dentistry and Oral Epidemiology
(3).
Additional surveys in the formerly-fluoridated towns of Spremberg and Zittau found. “Caries levels for the 12 -year-olds of both towns significantly decreased… following the cessation of water fluoridation.”
Not only did decay rates remain stable during an 11-month fluoridation break in Durham, NC, between September, 1990, and August, 1991 but dental fluorosis declined in children born during that period, according to the Journal of Dental Research
(4).
In British Columbia, Canada, “the prevalence of caries decreased over time in the fluoridation-ended community while remaining unchanged in the fluoridated community,” reported in Community Dentistry and Oral Epidemiology.
(5).
In 1973, the Dutch town of Tiel stopped fluoridation. Researchers counted drilled, missing, and filled tooth surfaces (DMFS) of Tiel’s 15-year olds, then collected identical data from never-fluoridated Culemborg. DMFS initially increased in Tiel then dipped to 11% of baseline from 1968/69 to 1987/8 8 while never-fluoridated Culemborg’s 15-year-olds had 72% less cavities over the same period, reports Caries Research.
(6).
A recently released government report out of Canada (7) shows similar negative results and offers a reason.
Fluoridation was launched in the 1940′s when dentists believed fluoride’s beneficial effects were achieved internally, through the bloodstream then absorbed inside the teeth. The Canadians report that “this effect is likely to be minor…The evidence for a post-eruptive (topical) effect… is much stronger.”
Therefore, swallowing fluoride doesn’t reduce tooth decay but does cause dental fluorosis — white spotted, yellow or brown stained and sometimes pitted teeth.
According to the ADA’s website “Dental decay can be expected to increase if water fluoridation in a community is discontinued for one year or more, even if topical products such as fluoride toothpaste and fluoride rinses are widely used.”
“Well, science proves the ADA is wrong about the claimed benefits of water fluoridation and they are wrong about the safety of water fluoridation, too” says lawyer Paul Beeber, President, New York State Coalition Opposed to Fluoridation. “Studies have linked fluoridation chemicals to increased blood lead levels, neurological defects, brittle bones, thyroid cancer and more,” says Beeber. “It’s time for the media to challenge the $cience that supports water fluoridation and present the truth to the public. We’ve made it easy for the media to access the ‘Medline’ [PubMed] abstracts via the links below. No more excuses.”
Other US government studies and statistics support the findings of these six studies and the Canadian government report. For example, children in fluoridated-since-1945 Newburgh, New York, have no less tooth decay but significantly more dental fluorosis than children from never-fluoridated Kingston, New York, according to Community Dentistry and Oral Epidemiology June 1999:
![]()
(1) “Caries trends 1992-1998 <tel:1992-1998> in two low-fluoride Finnish towns formerly with and without fluoridation,” Caries Research, Nov-Dec 2000 – Reference <http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=110930%2019&dopt=Abstract>
(2) “Caries prevalence after cessation of water fluoridation in La Salud, Cuba,” Caries Research Jan-Feb. 2000 — Reference <http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10601780&dopt=Abstract>
(3) “Decline of caries prevalence after the cessation of water fluoridation in the former East Germany, & quote; Community Dentistry and Oral Epidemiology, October 2000 — Reference <http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11014515&dopt=Abstract>
(4) “The effects of a break in water fluoridation on the development of dental caries and fluorosis,” Journal of Dental Research, Feb. 2000 — Reference <http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=10728978&dopt=Abstract>
(5) “Patterns of dental caries following the cessation of water fluoridation,” Community Dentistry and Oral Epidemiology, February 2001 — Reference <http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11153562&dopt=Abstract>
(6) “Caries experience of 15-year-old children in The Netherlands after discontinuation of water fluoridation,” Caries Research, 1993 — Reference <http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8519058&dopt=Abstract>

DENTAL FLUOROSIS – THE PSYCHOSOCIAL ISSUE ↓
→ Dental_Fluorosis_Book_Master ←
http://www.naturalnews.com/037089_coconut_oil_bacteria_tooth_decay.html#ixzz26W5jAFil

Julia Roberts – No toothpaste Smile
HAPPY ‘PRIMITIVE’ SMILES
DENTAL DISEASES – EXTRACTS FROM VARIOUS RESEARCH PAPERS:
-
Stunted children at 6 months of age were more likely to have non-emerged permanent molars at 6 years of age; Children from work social class families, those with height deficit for age at 12 months, child who did not attend day care center, brushing teeth less than once a day, and children with sweet consumption of at least once a day were risk factors for high level of primary dental caries at age six.
-
Non-nutritive sucking habits and digital sucking were the main risk factors for anterior open bite at age six.
-
Short breastfeeding and regular use of a pacifier were risk factors for posterior cross bite. Interaction between short duration of breastfeeding and the use of pacifier was also identified;
-
Dental caries at aged twelve was strongly and positively associated with dental caries at aged six.
-
The proportion of individuals with severe malocclusions at twelve years-old increased according to the number of malocclusions presented at six years-old;
-
Children who did not live with their biological father at birth, and children with higher dmf-t, reported a higher lifetime prevalence of toothache at age six years.
-
Population attributable risk for dental caries at age 12 were 3.1 % for deficit in height for age at twelve months and 64.9% for primary dental caries at age six.
-
The level of accuracy in predicting dental caries at age twelve by using life course socioeconomic, behavioral and clinical data was modest.
-
Dental caries are one of the most common chronic diseases world- wide. 90% of people have had dental problems or toothache caused by caries, and in low-to-middle income countries most caries remains untreated. Severe periodontitis affects 5–15% of most populations. Oral cancer is the eighth most common cancer worldwide and the most common in men in South East Asia. And 40–50% of people who are HIV positive have oral fungal, bacterial, or viral infections” (Lancet January 3, 2009)
Our Comments:
The above extracts from official dental research, highlights the importance of nutrition, but seems to avoiding referring to this, primitive tribes on their natural foods seem to have avoided most of these problems, certainly access to fresh wild food, rich in minerals and vitamins has been shown to provide good general health as well as dental health.
See: → ‘Hopewood Children’
“just say no to drugs”
FLUORIDATION AND STRONTIUM 90
→ tissue engineering. ←
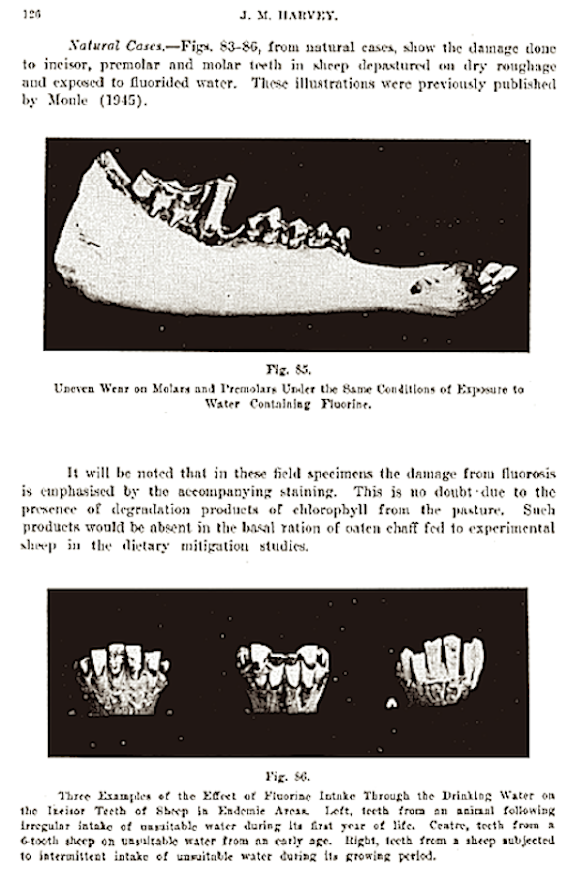
Fluoride delays tooth eruption and can be responsible for malocclusions, This delayed eruption caused by fluoride also occurs in sheep — see below ↓
See full text ↓ ↓ ↓
Queensland Government’s Research
![]()
HEALTH CONSIDERATIONS
There is evidence that long-term exposure to fluoride over 1.5 milligrams per litre may affect the development of healthy teeth in children up to six years, leading to dental fluorosis – a mottling of the teeth.
If the acceptable level is exceeded in circumstances where it is not practical to defluoridate the water supply, then parents are advised to use bottled water for children up to about six years of age, to limit or prevent dental fluorosis.
Another potential health consideration is skeletal fluorosis [a type of bone disease], which has occurred in association with high fluoride concentrations in drinking water [above 4 milligrams per litre], and also through occupational exposure to dust containing fluoride. It generally occurs after long-term exposure to high levels of fluoride [several years] and is reversible: if the exposure is removed, the fluoride levels in bones gradually decline.
South East Queensland’s water is regularly tested to ensure the level of these substances remains lower than those established by the guidelines.
Note: Other sources of fluorides are not considered…
Link to seqwater → HERE ←
— ROOT CANALS —
Information supplied by:

↓ ↓ ↓
97% of Terminal Cancer Patients Previously Had This Dental Procedure…
Story at-a-glance:
1.) During a root canal, there is no way to sterilize your tooth; after the root canal, dangerous bacteria hide out in the tooth and are unreachable with antibiotics
2.) Root-canaled and filled teeth harbor bacteria that morph into very toxic forms, which then can migrate to other tissues in your body and cause serious medical conditions, including diseases of your heart, kidneys, bones, and brain
3.) There is no other medical practice that permits leaving a dead body part inside your body, because it triggers your immune system to attack
4.) If you have a diseased tooth, or if you’ve already had a root canal,
I highly recommend consulting a biological dentist about have it extracted
Do you have a chronic degenerative disease? If so, have you been told,
“It’s all in your head?”
Well, that might not be that far from the truth… the root cause of your illness may be in your mouth.
There is a common dental procedure that nearly every dentist will tell you is completely safe, despite the fact that scientists have been warning of its dangers for more than 100 years.
Every day in the United States alone, 41,000 of these dental procedures are performed on patients who believe they are safely and permanently fixing their problem. What is this dental procedure?
The root canal.
More than 25 million root canals are performed every year in this country. [USA]
Root-canaled teeth are essentially “dead” teeth that can become silent incubators for highly toxic anaerobic bacteria that can, under certain conditions, make their way into your bloodstream to cause a number of serious medical conditions—many not appearing until decades later.
Most of these toxic teeth feel and look fine for many years, which make their role in systemic disease even harder to trace back.
Sadly, the vast majority of dentists are oblivious to the serious potential health risks they are exposing their patients to, risks that persist for the rest of their patients’ lives. The American Dental Association claims root canals have been proven safe, but they have NO published data or actual research to substantiate this claim.
Fortunately, I had some early mentors like Dr. Tom Stone and Dr. Douglas Cook, who educated me on this issue nearly 20 years ago. Were it not for a brilliant pioneering dentist who, more than a century ago, made the connection between root-canaled teeth and disease, this underlying cause of disease may have remained hidden to this day. The dentist’s name was Weston Price—regarded by many as the greatest dentist of all time.
Weston A. Price: World’s Greatest Dentist
Most dentists would be doing an enormous service to public health if they familiarized themselves with the work of Dr. Weston Pricei. Unfortunately, his work continues to be discounted and suppressed by medical and dental professionals alike.
Dr. Price was a dentist and researcher who traveled the world to study the teeth, bones, and diets of native populations living without the “benefit” of modern food. Around the year 1900, Price had been treating persistent root canal infections and became suspicious that root-canaled teeth always remained infected, in spite of treatments. Then one day, he recommended to a woman, wheelchair bound for six years, to have her root canal tooth extracted, even though it appeared to be fine.
She agreed, so he extracted her tooth and then implanted it under the skin of a rabbit. The rabbit amazingly developed the same crippling arthritis as the woman and died from the infection 10 days later. But the woman, now free of the toxic tooth, immediately recovered from her arthritis and could now walk without even the assistance of a cane.
Price discovered that it’s mechanically impossible to sterilize a root-canaled (e.g. root-filled) tooth.
He then went on to show that many chronic degenerative diseases originate from root-filled teeth—the most frequent being heart and circulatory diseases. He actually found 16 different causative bacterial agents for these conditions. But there were also strong correlations between root-filled teeth and diseases of the joints, brain and nervous system. Dr. Price went on to write two ground-breaking books in 1922 detailing his research into the link between dental pathology and chronic illness. Unfortunately, his work was deliberately buried for 70 years, until finally one endodontist named George Meinig recognized the importance of Price’s work and sought to expose the truth.
Dr. Meinig Advances the Work of Dr. Price
Dr. Meinig, a native of Chicago, was a captain in the U.S. Army during World War II before moving to Hollywood to become a dentist for the stars. He eventually became one of the founding members of the American Association of Endodontists (root canal specialists).
In the 1990s, he spent 18 months immersed in Dr. Price’s research. In June of 1993, Dr. Meinig published the book Root Canal Cover-Up, which continues to be the most comprehensive reference on this topic today. You can order your copy directly from the Price-Pottenger Foundationii.
What Dentists Don’t Know About the Anatomy of Your Teeth Your teeth are made of the hardest substances in your body.
In the middle of each tooth is the pulp chamber, a soft living inner structure that houses blood vessels and nerves. Surrounding the pulp chamber is the dentin, which is made of living cells that secrete a hard mineral substance. The outermost and hardest layer of your tooth is the white enamel, which encases the dentin.
The roots of each tooth descend into your jawbone and are held in place by the periodontal ligament. In dental school, dentists are taught that each tooth has one to four major canals. However, there are accessory canals that are never mentioned. Literally miles of them!
Just as your body has large blood vessels that branch down into very small capillaries, each of your teeth has a maze of very tiny tubules that, if stretched out, would extend for three miles. Weston Price identified as many as 75 separate accessory canals in a single central incisor (front tooth). For a more detailed explanation, refer to an article by Hal Huggins, DDS, MS, on the Weston A. Price Foundation website.iii (These images are borrowed from the Huggins article.)
Microscopic organisms regularly move in and around these tubules, like gophers in underground tunnels.
When a dentist performs a root canal, he or she hollows out the tooth, then fills the hollow chamber with a substance (called guttapercha), which cuts off the tooth from its blood supply, so fluid can no longer circulate through the tooth. But the maze of tiny tubules remains. And bacteria, cut off from their food supply, hide out in these tunnels where they are remarkably safe from antibiotics and your own body’s immune defenses.
The Root Cause of Much Disease
Under the stresses of oxygen and nutrient deprivation, these formerly friendly organisms morph into stronger, more virulent anaerobes that produce a variety of potent toxins. What were once ordinary, friendly oral bacteria mutate into highly toxic pathogens lurking in the tubules of the dead tooth, just awaiting an opportunity to spread.
No amount of sterilization has been found effective in reaching these tubules—and just about every single root-canaled tooth has been found colonized by these bacteria, especially around the apex and in the periodontal ligament. Often times, the infection extends down into the jawbone where it creates cavitations—areas of necrotic tissue in the jawbone itself.
Cavitations are areas of unhealed bone, often accompanied by pockets of infected tissue and gangrene. Sometimes they form after a tooth extraction (such as a wisdom tooth extraction), but they can also follow a root canal. According to Weston Price Foundation, in the records of 5,000 surgical cavitation cleanings, only two were found healed.
And all of this occurs with few, if any, accompanying symptoms. So you may have an abscessed dead tooth and not know it. This focal infection in the immediate area of the root-canaled tooth is bad enough, but the damage doesn’t stop there.
Root Canals Can Lead to Heart, Kidney, Bone, and Brain Disease
As long as your immune system remains strong, any bacteria that stray away from the infected tooth are captured and destroyed. But once your immune system is weakened by something like an accident or illness or other trauma, your immune system may be unable to keep the infection in check.
These bacteria can migrate out into surrounding tissues by hitching a ride into your blood stream, where they are transported to new locations to set up camp. The new location can be any organ or gland or tissue.
Dr. Price was able to transfer diseases harbored by humans to rabbits, by implanting fragments of root-canaled teeth, as mentioned above. He found that root canal fragments from a person who had suffered a heart attack, when implanted into a rabbit, would cause a heart attack in the rabbit within a few weeks.
He discovered he could transfer heart disease to the rabbit 100 percent of the time! Other diseases were more than 80 percent transferable by this method. Nearly every chronic degenerative disease has been linked with root canals, including:
• Heart disease
• Kidney disease
• Arthritis, joint, and rheumatic diseases
• Neurological diseases (including ALS and MS)
• Autoimmune diseases (Lupus and more)
There may also be a cancer connection. Dr. Robert Jones, a researcher of the relationship between root canals and breast cancer, found an extremely high correlation between root canals and breast cancer.iv He claims to have found the following correlations in a five-year study of 300 breast cancer cases:
• 93 percent of women with breast cancer had root canals
• 7 percent had other oral pathology
• Tumors, in the majority of cases, occurred on the same side of the
body as the root canal(s) or other oral pathology
Dr. Jones claims that toxins from the bacteria in an infected tooth or jawbone are able to inhibit the proteins that suppress tumor development. A German physician reported similar findings. Dr. Josef Issels reported that, in his 40 years of treating “terminal” cancer patients, 97 percent of his cancer patients had root canals. If these physicians are correct, the cure for cancer may be as simple as having a tooth pulled, then rebuilding your immune system.
Good Bugs Gone Bad
How are these mutant oral bacteria connected with heart disease or arthritis? The ADA and the AAE claim it’s a “myth” that the bacteria found in and around root-canaled teeth can cause diseasev. But they base that on the misguided assumption that the bacteria in these diseased teeth are the SAME as normal bacteria in your mouth—and that’s clearly not the case.
Today, bacteria can be identified using DNA analysis, whether they’re dead or alive, from their telltale DNA signatures.
In a continuation of Dr. Price’s work, the Toxic Element Research Foundation (TERF) used DNA analysis to examine root-canaled teeth, and they found bacterial contamination in 100 percent of the samples tested. They identified 42 different species of anaerobic bacteria in 43 root canal samples. In cavitations, 67 different bacteria were identified among the 85 samples tested, with individual samples housing between 19 to 53 types of bacteria each. The bacteria they found included the following types:
• Capnocytophagaochracea
• Fusobacteriumnucleatum
• Gemellamorbillorum
• Leptotrichiabuccalis
• Porphyromonasgingivalis
Are these just benign, ordinary mouth bugs? Absolutely not. Four can affect your heart, three can affect your nerves, two can affect your kidneys, two can affect your brain, and one can infect your sinus cavities… so they are anything BUT friendly! (If you want see just how unfriendly they can be, I invite you to investigate the footnotes.)
Approximately 400 percent more bacteria were found in the blood surrounding the root canal tooth than were found in the tooth itself, suggesting the tooth is the incubatorand the periodontal ligament is the food supply. The bone surrounding root-canaled teeth was found even HIGHER in bacterial count… not surprising, since bone is virtual buffet of bacterial nutrients.
Since When is Leaving A Dead Body Part IN Your Body a Good Idea?
There is no other medical procedure that involves allowing a dead body part to remain in your body. When your appendix dies, it’s removed. If you get frostbite or gangrene on a finger or toe, it is amputated. If a baby dies in utero, the body typically initiates a miscarriage.
Your immune system doesn’t care for dead substances, and just the presence of dead tissue can cause your system to launch an attack, which is another reason to avoid root canals—they leave behind a dead tooth.
Infection, plus the autoimmune rejection reaction, causes more bacteria to collect around the dead tissue. In the case of a root canal, bacteria are given the opportunity to flush into your blood stream every time you bite down.
Why Dentists Cling to the Belief Root Canals are Safe
The ADA rejects Dr. Price’s evidence, claiming root canals are safe, yet they offer no published data or actual research to substantiate their claim. American Heart Association recommends a dose of antibiotics before many routine dental procedures to prevent infective endocarditis (IE) if you have certain heart conditions that predispose you to this type of infection.
So, on the one hand, the ADA acknowledges oral bacteria can make their way from your mouth to your heart and cause a life-threatening infection.
But at the same time, the industry vehemently denies any possibility that these same bacteria—toxic strains KNOWN to be pathogenic to humans—can hide out in your dead root-canaled tooth to be released into your blood stream every time you chew, where they can damage your health in a multitude of ways.
Is this really that large of a leap? Could there be another reason so many dentists, as well as the ADA and the AAE, refuse to admit root canals are dangerous? Well, yes, as a matter of fact, there is. Root canals are the most profitable procedure in dentistry.x
What You Need to Know to AVOID a Root Canal
I strongly recommend never getting a root canal. Risking your health to preserve a tooth simply doesn’t make sense. Unfortunately, there are many people who’ve already have one. If you have, you should seriously consider having the tooth removed, even if it looks and feels fine. Remember, as soon as your immune system is compromised, your risk of of developing a serious medical problem increases—and assaults on your immune system are far too frequent in today’s world.
If you have a tooth removed, there are a few options available to you.
1.) Partial denture: This is a removable denture, often just called a “partial.” It’s the simplest and least expensive option.
2.) Bridge: This is a more permanent fixture resembling a real tooth but is a bit more involved and expensive to build.
3.) Implant: This is a permanent artificial tooth, typically titanium, implanted in your gums and jaw. There are some problems with these due to reactions to the metals used. Zirconium is a newer implant material that shows promise for fewer complications.
[Editor: ceramic implants are a more recent option]
But just pulling the tooth and inserting some sort of artificial replacement isn’t enough.
Dentists are taught to remove the tooth but leave your periodontal ligament. But as you now know, this ligament can serve as a breeding ground for deadly bacteria. Most experts who’ve studied this recommend removing the ligament, along with one millimeter of the bony socket, in order to drastically reduce your risk of developing an infection from the bacterially infected tissues left behind.
I strongly recommend consulting a biological dentist because they are uniquely trained to do these extractions properly and safely, as well as being adept at removing mercury fillings, if necessary. Their approach to dental care is far more holistic and considers the impact on your entire body—not JUST your mouth.
If you need to find a biological dentist in your area, I recommend visiting toxicteeth.orgxi, a resource sponsored by Consumers for Dental Choice. This organization, championed by Charlie Brown, is a highly reputable organization that has fought to protect and educate consumers so that they can make better-informed decisions about their dental care. The organization also heads up the Campaign for Mercury-Free Dentistry.
References: Source: Video Transcript
Related Links:
Using Primitive Wisdom to Radically Improve Your Health
Is Your Dentist Drilling for Dollars?
Ignore This Simple Daily Habit and Watch Your Risk of Heart Disease Soar by 70%
Thank you Dr. Mercola!
The Dramatic Benefits of Minimally Invasive Dentistry by Dr. Mercola 24 February 2013
→ Visit the Mercola Video Library ←
Dental health is an important part of your overall health.
Unnecessary drilling and filling your teeth with toxic materials can have far-reaching, long-term health ramifications.
Fortunately, there are options, but it can be tricky finding a dentist that is fully familiar with alternative types of dentistry, such as minimally invasive dentistry and biomimetic dentistry – the latter of which means ‘mimicking nature,’ and involves using tooth restorations and techniques that imitate natural teeth, both in appearance and function.
Both of these are covered in Carol Vander Stoep’s book, Mouth Matters. Carol has been a dental hygienist for 25 years.
She chose a career in dental hygiene over dentistry because she valued prevention over repair, and her book can be a valuable resource for lay-persons and dentists alike. It discusses whole body health from a dental perspective, along with advanced forms of dental diagnosis and treatment that we should all be requesting from our dentists.
“When I wrote the first edition of Mouth Matters, it was all about how gum disease affects heart disease, diabetes, stroke risk – all of those degenerative diseases of the body. I wasn’t all that interested in teeth.”
Carol says, “What I started to realize, as the question of root canals and breaking down teeth started to surface, was that if a tooth does break down or catastrophically fail, you’re facing the same issue about introducing germs back into the body.
As a result of having written the first edition, it was wonderful for me to be able to be introduced to some of the top dental researchers, clinicians, people who are really trying to start a revolution in dentistry and trying really hard to do it.
But we all know that revolutions don’t start from the top-down; they have to start from the bottom-up. That’s why I’m here today. Because really, we need to educate people as to what it is that we want in dentistry. We need to know the kind of care that we want.”
Naturally, preceding technological developments in dental tools is the foundation of diet. If you get your diet right, which includes avoiding sugars, processed foods and grains, then you’re creating an environment in your mouth that will be resistant to dental decay.
Fermented foods, such as fermented vegetables, can be tremendously beneficial for your oral health. I’ve had a significant problem with tartar buildup on my teeth, having to get a cleaning once a month. Once I added fermented vegetables to my diet, I’ve been able to extend it to every two months. So diet is really the foundation of healthy teeth and gums.
Modern Dentistry Really Isn’t as Advanced as it Could Be
Modern dentistry is still fairly primitive in many ways. About half of American dentists still use amalgam, half of which is neurotoxic mercury – not silver as the name “silver fillings” would imply.
But that’s not the only problem. The act of drilling into a tooth is in and of itself very destructive to the tooth, especially when using a high speed drill. It can create tiny little cracks that lead to further deterioration of the tooth over time. Low-speed drilling is not as destructive to the tooth but is still far from optimal.
The conventional strategy to “drill and fill,” regardless of the restorative material used, is an impermanent solution. An estimated 70-80 percent of the work done by dentists is re-repairing previous dental work.
“It’s important to really understand – and one thing that I didn’t appreciate was – that teeth are one of the most complex structures in your body,” Carol says. “It takes a full nine years for them to even form. It’s a series of arches.
If you would think about masonry, anytime you cut an opening in masonry in order to handle the compress of strengths, a mason has to build an arch to hold that strength. If you were to take the keystone out of that arch or to cut the leg out off of that arch, the whole arch would collapse; the whole structure would collapse.
What I think is so beautiful about a tooth – an adult molar – is that it is a series of arches. There are at least four to five arches built into the tooth. They’re actually made of different layers.
You have an outer, very tough shell called enamel. That’s only two percent organic, and it doesn’t flex a lot. But the internal part of the tooth, the body of the tooth, is 55 percent organic. It’s made of collagen and water. It’s made to shake, rattle, and roll, as we put all these compressive strengths on it. Chewing is a very, very tough thing. We want these teeth to last a hundred years and stay in function, and they’re designed to do that.”
The concept of minimally invasive dentistry is still in its infancy, although Dr. Tim Rainey has been tirelessly lecturing on the subject, all over the world, for the last 25 years. He has also written about it in dental journals. He still has a dental practice in Refugio, Texas where the majority of his patients are underprivileged children on Medicaid.
“The beauty of this dentistry is that it doesn’t require shots. It doesn’t take a lot of time. It’s not painful. In fact, since he introduced ozone into his practice, he has never had a child come in with an asymptomatic tooth (meaning a tooth in pain) that has ever needed a root canal or an extraction. He’s never even needed to anesthetize them,” Carol says.
The Importance of Early Diagnosis
Early diagnosis is essential if you want to avoid invasive restorations. Unfortunately, conventional dentistry still has a lot to learn in this respect. According to Carol, traditional means of diagnosis, using an explorer, and x-rays only have a 25 percent success rate in terms of accurate diagnosis.
False positives and false negatives can occur and do so quite frequently. Carol explains:
“You can have a tooth to be completely stain-free… It cannot stick with an explorer. If we take an X-ray of the tooth, nothing shows up. It looks completely pristine.
However, [decay] can be hiding up under those pits and grooves – some rather significant decay. In fact, when the enamel is forming, a lot of times there are little folds, fractures, and not completely mineralized enamel. There are defects in the enamel that we can’t catch for many, many years. You can’t really diagnose or treat an unopened fissure. That’s really the first most important thing – I think – that people need to know.
…The decay has to get pretty deep into the tooth before we can diagnose it. In fact, X-rays are very late-stage diagnosis. Decay has to be at least two millimeters into the second layer of tooth under the enamel before an X-ray can begin to catch it. Then you have to be much more invasive in treating it. You want to be able to catch diagnosis early.”
Fluoride is commonly thought to be a primary prevention strategy against tooth decay, despite the fact that, like mercury fillings, it is a highly toxic substance, shown to lower IQ in children. According to Carol, fluoride also makes early diagnosis more difficult.
“When that outer shell is heavily infused with fluoride, it changes the way an X-ray goes through a tooth,” she says. “I think it delays diagnosis, because we’re not able to see that decay as easily.”
There are Better Alternatives to Crowns
Eventually, after a tooth has been repaired a number of times, a crown typically becomes necessary. However, biomimetic dentistry offers excellent alternatives to crowns.
“There are principles of adhesive dentistry that dentists should know, but again, most of them don’t know. There are six different ways to put [resin material] in to where it can recreate the tooth structure,” Carol explains.
For example, the dentist can section the resins, layering the material in according to something called C-factor (which has to do with the shrinkage of the material), so that it’s not creating too much pressure on the tooth in any direction. Another alternative is to use more expensive inlays or onlays. A CEREC® machine can cut the material into precise-fitting pieces that are then permanently adhered into the cavity. CEREC® material can also be used to replace an entire tooth, like a crown. However, CEREC® inlays and crowns are far better than other resin fillers and metal or porcelain crowns as they are permanent and will not need to be replaced with time.
The Benefits of Ozone in Dentistry
Now, most people get concerned when they hear ozone, equating it with ozone pollution. When ozone levels rise, we’re likely to get sick. But this is due to the pollutants caught in the ozone – ozone itself is actually nature’s way of cleaning the air. Granted, ozone gas, by itself, should not be breathed as it’s toxic to lung tissue in high concentrations. But when selectively applied, it can provide significant benefits in dentistry. In fact, according to Carol, ozone is the only way to predictably re-mineralize the tooth. The conventional thought is that this is the function of fluoride, but this is not true.
Another component of minimally invasive dentistry is the use of ozone. “I can’t believe I didn’t hear of ozone until about a year and a half ago,”
Carol says. “But it’s wonderful.”Fluoride actually has a powerfully detrimental effect, because while it can strengthen the tooth, that’s not the most important factor in preventing decay. While making the enamel denser, it also makes it more brittle by destroying the surface crystal matrix that helps protect the tooth. It’s a very similar process as osteoporosis drugs that make your bones denser but more brittle…
“We are using it close to the mouth, so there are precautions that you have to know,” Carols says. “You have to take a course in it. You can’t just start using it. But since we deal with microbes in the mouth, I can’t imagine a better place for ozone. I use it all the time in gum disease.
…The beauty is, with ozone, you don’t have to remove all the decayed material. You just remove the worst of it, then you hit it with ozone. If there are any dentists listening, they can take it down just to what we call the leathery layer. There’s still plenty of structure there. The crystalline structure is still there, and it’s still strong. It’s just been infiltrated by bacteria and their end products.
In the old way, you would want to take all of that out. We don’t want to do that. Leave that there. Hit it with ozone for a few minutes and change the chemistry of the tooth. Let it re-harden. If you don’t fill it, it will take about two months to re-harden. If you fill it, it takes four months to re-harden. It’s kind of a lovely concept, isn’t it?
…Ozone is the only way to predictably re-mineralize the tooth – it’s a component of the process. Because what it’s going to do [when applied in gas form], is diffuse into the tooth, through those little white spots into the tooth… First, it’s going to kill all the microbes in the tooth. That’s important… The end products of bacteria are acids. It changes the chemistry of the tooth from acid to neutral, so that now the tooth can re-mineralize the way it’s supposed to.
A lot of people think that re-mineralization happens from the outside in, but most of that re-mineralization is actually going to be coming through the pulp. The pulp, of course, is that hollow internal structure of a tooth that is filled with blood vessels and nerves and is designed to give the tooth nutrients and keep it hydrated. The minerals are going to come in through the pulp, feed out this way, bring the minerals to that area, and harden it.”
Everyday Dental Hygiene Tips
If you’re like most people, you probably use toothpaste. But according to Carol, not only do you not need fluoridated toothpaste, you don’t need any toothpaste at all. This is because plaque is removed through mechanical scrubbing, and the toothpaste might just give you a false sense of “clean.”
“Many of these toothpastes have surfactants and things that keep the tongue from telling you when it’s clean. If it still feels like a sweater’s on your tooth, it is. Also, you can tell better if you’re jiggling it under the gums. That’s an important feedback for you to know,” she says.
“I have people using the toothbrush as long as it takes to where the teeth feel nice and smooth. If they want to add those adjuncts, I have them use baking soda at night because that’s when our saliva slows down, and we really want to raise that pH. It’s going to have a longer effect.”
Another interesting tip is to use ozonated oil. This is simply olive or jojoba oil through which ozone has been bubbled through (note it must be medical grade ozone). You can use it to brush your teeth with, or apply it to your gums with a toothpick. (One caveat is that it doesn’t taste good.)
“My favorite tool might be the butler soft picks… It’s just a little tool that I can dip in the ozonated oil and put in between my teeth. You can put it anywhere there’s a plaque. It pretty much melts the plaque off,” Carol says.
More Information
For more information, please read Carol’s book, Mouth Matters. You may also want to recommend it to your dentist. After all, the only way dentistry will change is by patients asking for better alternatives. You can also find more information on her website, mouthmattersbook.com.
“You can say, ‘this is the kind of dentistry I want,’” Carol says. “Then also, for those who don’t have a dentist, I have developed a database. I thought that was really important to do, so that people can go to see who it is that’s been trained in it, who are using it, who are doing biomimetic dentistry, and who are using ozone in their practices. Ideally, it’s a marriage of all three.”
Alternatives such as CEREC® inlays are taught at the University of Southern California under Pascal Magne and Dave Alleman, and dental applications for ozone therapy are taught by Mollica & Harris (for information oxygenhealingtherapies.com).
Thank you Dr. Mercola!
MORE SURVEYS
An analysis of the skulls of more than 300 Roman Britons has found
a significantly lower rate of periodontitis, a common form
of gum disease, than exists in today’s population.
↓ BBC ↓
ROMANS’ TEETH BETTER THAN MODERN BRITONS’
It wasn’t just British roads that were straighter in Roman times: smiles were, too.
For all Britain’s access to modern dentistry, flossing and mouthwash, a study published yesterday has found that the buffed and brushed mouths of 21st-century Britons are still more likely to harbour gum disease than those of their third-century forebears.
An analysis of the skulls of more than 300 Roman Britons has found a significantly lower rate of periodontitis, a common form of gum disease, than exists in today’s population. Among those examined — who were originally buried in a site in Poundbury, Dorset — between 5 per cent and 10 per cent had the disease, compared with about 15 per cent to 30 per cent today.
However, they also had considerably more evidence of abrasion on their teeth, probably a result of the diet of coarse grains that was common.
The work involved looking at the sockets holding the teeth into the jaw.
“Because gum disease causes disruption of the bone around the teeth, we are able to measure it,” said Francis Hughes, professor of periodontology at King’s College London.
He and his colleagues analysed a large collection of skeletons held at the Natural History Museum from the Poundbury burial site.
“To a lot of people’s surprise they had quite a lot less periodontitis than the modern human population. It was about a third as common as today,” Professor Hughes said.
Some of the explanation for this does not exactly provide cause for envy: the ancient Britons contracted even more serious diseases first, and died of those instead of suffering through old age with bad teeth.
The most common age at death appeared to be in the 40s.
The reason for the modern mouth to be less healthy than it was centuries ago is probably a result of two things — diabetes and smoking. “Those two change the risk enormously,” Professor Hughes said.
Periodontitis starts as gingivitis, a consequence of poor brushing that often manifests as bleeding and inflamed gums. This response is actually a protective mechanism.
“It’s the body trying fight the bacteria off. In smoking and diabetes that protective mechanism is decreased — the body is less able to fight,” Professor Hughes said.
Starting with bleeding, the disease progresses through receding gums, looseness of teeth and eventually tooth loss.
With a life free not just from smoking and diabetes but also from refined sugar, the Poundbury teeth were similarly less affected by cavities. Nevertheless, the research, published in the British Dental Journal, did not find that the oral hygiene of ancient Britons was something to be aspired to.
“Decay was not widespread like it might be today,” Professor Hughes said. “But it was still there, probably a consequence of the starchy cereals they ate. That increased bacterial growth.”
Some decay went unchecked. Some teeth had decayed to the point where they had infected the nerve and others caused holes down to the jaw itself.
“The amount of chronic infection must have caused a lot of misery,” Professor Hughes said. His profession would have been in demand even in that day and age, he said. “It’s still a rather good advert for dentists.”
The Times
![]()
![]()
