Global Decline in Tooth Decay
correlates with reduced Airborne Lead
(Pb) but water Fluoridation prevents further progress.
Geoff PainNovember 2017Abstract:The observed large reduction in dental caries incidence worldwide since the 1970s is shown to correlate with reduction in airborne Lead due to phase-out of Tetraethyl Lead use in gasoline. This accounts also for the fact that there is no discernible difference in dental decay rates between nations that suffer Fluoridation and those where it is banned. The deliberate addition of Lead as a major contaminant of phosphate fertilizer industrial waste used in Fluoridation plus the exacerbation of Plumbosolvency by Fluoride must cease if further reduction in tooth decay and co-morbidity is to be accomplished.
Keywords: Caries, Decay, Fluoridation, Fluoride, Fluorosis, Gasoline, Hypoplasia, IQ,
Lead, Neurotoxin, Petrol, Plumbosolvency, Teeth, and Violence.
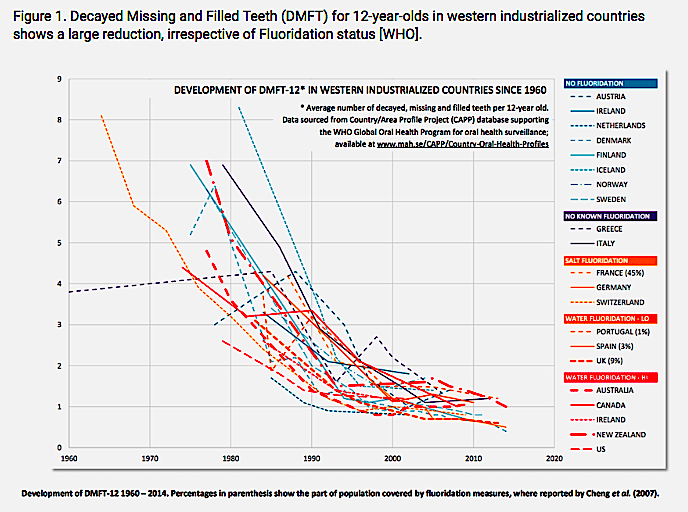
Introduction Proponents of disposing of phosphate fertilizer industrial waste, contaminated with light and heavy metals including Lead (up to 100 mg/kg) in mass medication, called water Fluoridation, falsely claim that it has reduced tooth decay [Kumar 1998]. Numerous authors have demonstrated the absurdity of this claim by pointing to the observed large reduction in dental caries incidence worldwide since the 1970s [Figure 1, WHO]. There is no discernible variation in dental decay rates with national Fluoridation status, as measured by Decayed, Missing or Filled Teeth (DMFT) shown in Figures 1 to 4 [WHO, Leverett 1982, Diesendorf 1986, 1988, 1990, Colquhoun 1993, 1997]. Figure 1. Decayed Missing and Filled Teeth (DMFT) for 12-year-olds in western industrialized countries shows a large reduction, irrespective of Fluoridation status [WHO]. Figure 2. Decline in dental caries incidence in communities with non-fluoridated water [Leverett 1982]. Figure 3. Decline in the average number of permanent teeth with caries in Australian states from 1977 to 1983, a period when Lead air emissions from fuel were being reduced. Note that Queensland exhibited declining tooth decay and was not subject to Fluoridation [Diesendorf 1986]. Figure 4. Decline in decay in deciduous teeth of 5-year-olds in New Zealand from 1930 to 1990 showing no discernible influence of Fluoride toothpaste or the introduction of water Fluoridation on the trend [Colquhoun 1997]. Some reports have suggested that the general decline in decay shown in Figure 1 has slowed or reversed in the United States and elsewhere [Burt 1994, Downer 1994, Beltran 2005]. For Australia the trend line in Figure 1 suggests the decay incidence among young children is increasing. Decay rates of primary teeth across children of all age groups increased during the period from 1996-1999, reversing the trend which saw a decline in rates of decay during 1991-1996. The trend since 1996 was most significant for five-year-old children who experienced a 21.7% increase in decay during this period [ADA 2007] in a period when Fluoridation was expanding.
The prevalence and severity of dental caries in the United States decreased substantially from 1971 to 1999 [Burt 1999]. National surveys reported that the prevalence of any dental caries among children aged 12-17 years declined from 90.4% in 1971-1974 to 67% in 1988-1991. DMFT declined from 6.2 to 2.8 during this period [NIDR 1981, Kelly 1979, NIDR 1989, Kaste 1996]. At the same time tooth damage from Fluorosis increased dramatically [Ko 2015]. After communal water fluoridation was discontinued in several communities in the former East Germany [Künzel 2000], Cuba and Finland, caries prevalence remained stable or continued to fall and did not rise as had been anticipated [Newbrun 2010]. Australian Government Failure to acknowledge International Trends. The toxic risks and rapid decline in dental disease independent of water Fluoridation led to cessation of Fluoridation in numerous jurisdictions [Ayoob 2006, Fagin 2008, Kalsbeek 1993].
The Australian National Health and Medical Research Council (NHMRC) failed to acknowledge the implications of the global trend of declining tooth decay and actively promotes the use of phosphate fertilizer industry waste in water Fluoridation. In 2007 the NHMRC specifically excluded from consideration many peer-reviewed scientific papers discussing the trend of declining decay, including: Birkeland 2000, Birkeland 2001, Birkeland 2002, Bratthall 1996, Carvalho 2001, der Fehr 1997, de Liefde 1998, Gillcrist 1996, Hac 1997, Haugejorden 1996, Krasse 1996, Lo 1997, Petersson 1996, Vrbic 2000, Ziegelbecker 1998. Fluoride does not work topically.
Fluoride varnish has been shown to be useless when it was used as a public health intervention in the hope of preventing caries in the first permanent molar teeth [Milsom 2011]. Brushing with Fluoride toothpaste causes Fluorosis [Wong 2010] leading to the major toothpaste vendor Colgate offering Fluoride free toothpaste for children that is now designated “safe to swallow”. Lead exposure reduction as the Major Factor in Tooth Decay Decline Humans have suffered severe dental defects caused by Lead exposure for centuries. Examination of 486 skulls with complete dentitions from 3rd – 5th century AD Romano-Britons from the cemetery in Poundbury, Dorset, UK showed that they suffered excess Lead ingestion, poor diet and recurrent infections resulting in anomalies in tooth number, crown size and shape, root morphology and deposition of enamel matrix [Koh 2014]. Scanning electron microscopy revealed deep, wide cracks in the occlusal enamel of Lead intoxicated rats and molar size was reduced in line with studies of the ancient Romans [Chen 2012].
Lead exposure causes hypoplasia in deciduous teeth of children [Brudevold 1956, 1977, Lawson 1971]. Blood lead level was positively associated with number of caries among urban children, even with adjustment for demographic and maternal factors and child dental practices. The association was stronger in primary than in permanent dentition. Children with blood lead levels of ≥ 4 μg/dL had, on average, two more decayed surfaces than did children with a blood lead level of 1 μg/dL, an increase of approximately 20% [Gemmel 2002, Martin 2007].
In humans, Lead, like Fluoride, is accumulated and stored in bones [Capar 1979] with a half-life of approximately 62 years [Watson 1997]. That Lead can be remobilized during pregnancy and is available to damage the mother and her foetus [Gil 1990, 1995]. The strength of Lead binding to Hydroxyapatite lead some researchers to recommend the use of Lead Fluoride in dental prevention, claiming that lead was more effective than Fluoride alone [Buonocore 1945]. Mothers pass on ingested or inhaled Lead to the foetus and through concentration in breast milk [Chen 2012]. In rats, levels of Lead in milk from Lead-treated dams were approximately 10 times as high as the corresponding blood Lead levels [Watson 1997]. Lead continues to accumulate [Gil 1994, 1996] in the growing deciduous tooth of the infant and the amount found matches airborne Lead levels. Rural areas demonstrate much less contamination [Figure 5, Stewart 1974]. High Lead levels were found in extracted teeth from Irish children [O’Mullane 2007]. Figure 5. Lead measured in deciduous teeth increases with age [Stewart 1974]. The so-called “Lead Line” ♦ in teeth is an unsightly indicator of an acute exposure to Lead. It was found not to contain significant Lead but instead was shown to consist of continuous hypomineralized interglobular spaces within the dentine.
It was suggested that the Lead Line results from damage to the odontoblasts and other hard tissue-forming cells producing a rapid loss of intracellular calcium temporarily displaced by lead ions and a subsequent disturbance of local calcium metabolism [Appleton 1991]. Earlier it was shown that an acute dose of Lead results in increased serum Calcium and Phosphorus levels a short time after injection as a result of Lead attack on bone [Kato 1978]. During the period 1980 to 1998, WHO data for developing countries, many of which were still using Lead in fuel, showed mean DMFT increased from about 1.8 to about 2.3 [Petersen 2003]. Comparisons of caries-free children versus those with some caries among children 5 to 17 years of age showed that a 5-μg/dL change in blood lead level was associated with an elevated risk for caries (odds ratio, 1.8; 95% confidence interval, 1.3-2.5) [Moss 1999, Campbell 2000]. It was estimated that approximately 2.7 million excess cases of dental caries in older children and adolescents may be attributable to environmental Lead exposure itself or a factor that is directly linked to environmental lead exposure [Moss 1999]. A strong independent association between blood Lead levels of young children aged 2 to 6 years and the extent and severity of caries has been found [Wiener 2015]. Recent work from Korea looking at deciduous teeth, found a dose-dependent increase in decayed and filled surfaces with increasing blood lead levels with a prevalence ratio of 1.14 (95% confidence interval: 1.02-1.27) [Kim 2017]. Earlier work found prevalence of dental caries among Korean children was 30.4% in 8-year-olds in deciduous teeth and 57.3% in 12-year-olds in permanent teeth in 2012 [KNOHS]. The mean blood lead levels were 1.34, 1.26, and 1.14 μg/dL in Korean children aged 3–5, 6–11, and 12–18 years, respectively, from 2012 to 2014 [Burm 2012], which were higher than the 0.838 and 0.680 μg/dL in US children aged 6–11 and 12–19 years, respectively, from 2009 to 2010 [CDC 2009 cited in Kim 2017]. Exposure to lead, prenatally and perinatally, results in high rates of dental caries in laboratory rats [Watson 1997]. In the study, female rats were exposed to 34 ppm of lead in drinking water as young adults, during pregnancy, and during lactation. After 5 weeks, pups born to the lead-exposed rats had significantly more dental caries lesions than controls. Lead exposure resulted in an almost 40% increase in the prevalence of caries and a decrease in stimulated parotid function of nearly 30%. Reduction in saliva, or “dry mouth syndrome” is a known risk for dental caries. Global action to phase-out or ban the use of Tetraethyl Lead as a fuel antiknock agent, except for piston engine aircraft, was initiated by the undeniable fact that Lead is a neurotoxin [Canfield 2003, Bandeen-Roche 2009] demonstrating dose-dependent reduction of IQ [Figure 6, Needleman 1979], elevated attention deficit and violent crime. Leaded gasoline for motor vehicles is still sold in Afghanistan, Algeria, Iraq, Myanmar, North Korea and Yemen. In the United States, analysis of three surveys of blood Lead showed the effect of rapidly reducing the use of Lead in fuels. Mean blood lead level for ages 1 to 74 years dropped 78%, from 12.8 to 2.8 μg/dL. Mean blood lead levels of children aged 1 to 5 years declined 77%, from 13.7 to 3.2 μg/dL, for non-Hispanic white children and 72%, 20.2 to 5.6 μg/dL, for non-Hispanic black children. The prevalence of blood lead levels 10 μg/dL or greater for children aged 1 to 5 years declined from 85.0% to 5.5% for non-Hispanic white children and from 97.7% to 20.6% for non-Hispanic black children. The study did not consider plumbosolvency due to Fluoridation or water Lead levels [Pirkle 1994]. Figure 6. Demonstration of IQ reduction by the neurotoxin Lead was clear [Needleman 1979].Figure 7. Phase-out of Lead in fuel in European and Scandinavian countries 1985 to 1997 [Löfgren 2000].
The differences in phase-out plans for a number of countries as shown in Figure 7 might help in understanding minor differences in observed dental decay rates over time in Figure 1. We see that the order of achieving close to complete phase-out or ban of Lead in motor fuel appears in Figure 7 as: Austria 1993, Denmark, Finland, Germany and Sweden around 1994, Netherlands around 1998. Other countries were slower, including Portugal 1999, France and UK 2000, Greece 2002. Lead concentrations measured in Greenland snow decreased by a factor of 7.5 over a 20-year period from the late 1960s due to this phase-out [Boutron 1991]. In Figure 8 the phase-out by Australian state is shown [Kristensen 2015} however there were variations within states allowing use of Lead in rural areas for extended periods compared to the densely populated cities Figure 8. Emissions of Lead to atmosphere 1933 to 2002 in Australian States [Kristensen 2015]. The reduction in atmospheric Lead was accompanied by a reduction in brain damage and associated violent crime Figure 9, Nevin 2000, Drum 2016]. Note the shift of 23 years after the corresponding prenatal exposure and also maintenance of violent crime rate at almost 3 times the 1937 rate after the major reduction in airborne Lead from fuel.
It has been observed that part of the Lead deposited historically is still available from inhaled legacy contaminated soil with caries levels elevated in Lead contaminated areas of Thailand [Youravong 2006]. Lead from contaminated food and water is still a major public health problem. Figure 9. Incidence of violent crime (in brown), versus the amount of atmospheric Lead from fuel (in blue) overlaid with a shift of 23 years after the corresponding prenatal exposure [Drum 2016, Nevin 2000]. Synergy of Lead and Fluoride in causing Tooth Damage A review of evidence linking heavy metal pollution with substance abuse and crime, including presentation of data linking the ban on sales of leaded gasoline with decline in crime 16 years later, also linked Fluoridation to Lead and crime levels [Masters 1999]. Geographical data analyses contradicted the “null hypothesis” that there is no difference in the effects of sodium fluoride and the silicofluorides.
Analysis of a US national sample of over 4,000 children in NHANES III, showed that water fluoridation is associated with a significant increase in children’s blood lead, with especially strong effects among minority children [Coplan 1999]. This Fluoride enhanced Plumbosolvency is discussed in more detail elsewhere [Pain 2015]. It has been shown that Lead exacerbates dental Fluorosis in rodents [Leite 2011]. Lead was earlier shown to inhibit proteinolysis when a crude enamel extract containing enamel proteases was tested in vitro. The mechanism of Lead interference with amelogenesis is most likely due to alteration in normal proteolysis [Gerlach 2000, 2002]. Fluoride increases the Lead level in blood and in calcified tissues of rodents [Sawan 2010]. Figure 10. Australian median Lead levels in children have not declined since the final cessation of the use of Lead in motor fuel in 2002, indicating Lead from water, food and contaminated soil are still producing unacceptable poisoning of the general population [Taylor 2014]. Most of the world recognizes that the only safe level of Lead is Zero, however Australian agencies including the NHMRC, Food Standards Australia and New Zealand (FSANZ), the Therapeutic Goods Administration (TGA) and the Australian Institute of Health and Welfare have been reluctant to coordinate systematic data collection including blood analysis or to lower allowable or action levels for Lead [Taylor 2014].
Their continued endorsement of deliberate Lead contamination through water Fluoridation prevents them from trying to achieve the Zero target. Conclusion Reduction of airborne Lead pollution following the phase-out of Tetraethyl Lead in motor fuel is the most plausible explanation for the very large observed global reduction in decay rates and the fact that there is no discernible difference in dental decay rates versus national Fluoridation status. The deliberate addition of Lead as a major contaminant of phosphate fertilizer industrial waste used in Fluoridation plus the exacerbation of Plumbosolvency caused by Fluoridation must cease if further reduction in blood Lead levels and tooth decay is to be accomplished. It is time for the governments of the few remaining countries where Fluoridation persists to place an immediate ban on the practice and force industry to permanently immobilize their toxic waste. The fact that WHO now rates Fluoride as more toxic than Lead should be a wake-up call to politicians every where. Lead target level of Zero should drive coordinated policy and planning.
Ending Fluoridation is a simple and cheap firststep toward achieving better dental, mental and general health. References ADA – Aust Dental Association. 2007. Research funding to fight childhood tooth decay. Wednesday, 18 July. Appleton J. 1991. The effect of lead acetate on dentine formation in the rat. Archives of Oral Biology 36(5):377-82. Ayoob S, Gupta AK. 2006. Fluoride in Drinking Water: A Review on the Status and Stress Effects. Critical Reviews in Environmental Science and Technology 36:(6):433-487. Bandeen-Roche K, Glass TA, Bolla KI, Todd AC, Schwartz BS. 2009. Cumulative lead dose and cognitive function inolder adults. Epidemiology 20:831-39. Beltrán-Aguilar ED, Barker LK, Canto MK, Dye BA, Gooch BF, Griffin SO, Hyman J, Jaramillo F, Kingman A, Nowjack-Raymer R, Selwitz RH, Wu T. 2005. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism, and Enamel Fluorosis – United States, 1988-1994 and 1999-2002. Morbidity and Mortality Weekly Report. Surveillance Summaries August 26 54(03):1-44. Buonocore MG, Bibby BG. 1945. The effect of various ions on enamel solubility. J Dent Res 24(2):103-108.Birkeland JM, Haugejorden O, der Fehr FR. 2000. Some factors associated with the caries decline among Norwegian children and adolescents: age-specific and cohort analyses. Caries Research, 34(2):109-116. Birkeland JM, Haugejorden O. 2001. Caries decline before fluoride toothpaste was available: earlier and greater decline in the rural north than in south western Norway. Acta Odontologica Scandinavica 59(1):7-13. Birkeland JM, Haugejorden O, der Fehr FR. 2002 Analyses of the caries decline and incidence among Norwegian adolescents 1985-2000. Acta Odontologica Scandinavica 60(5):281-289.Boutron CF, Görlach U, Candelone J-P, Bolshov MA, & Delmas RJ. 1991. Decrease in anthropogenic lead, cadmiumand zinc in Greenland snows since the late 1960s. Nature (Lond) 353:153-156.Bratthall D, Hansel-Petersson G, Sundberg H. 1996 Reasons for the caries decline what do the experts believe? Eur JOral Sci 104:416- 422 excluded Brudevold F, Steadman LT. 1956. The distribution of lead in human enamel. J Dent Res. 35:430-437. Brudevold F, Aasenden R, Srinivasian BN, Bakhos Y. 1977. Lead in enamel and saliva, dental caries and the use of enamel biopsies for measuring past exposure to lead. J Dent Res. 56:1165-1171.Burm E, Song I, Ha M, Kim YM, Lee KJ, Kim HC, et al. 2016. Representative levels of blood lead, mercury, and urinary cadmium in youth: Korean Environmental Health Survey in Children and Adolescents (KorEHS-C), 2012–2014. Int JHyg Environ Health. 219(4–5):412–8. Cited in Kim 2017. Burt BA, Eklund SA. Dentistry, dental practice, and the community. 5th ed. Philadelphia, PA: W.B. Saunders, 1999. Burt BA. 1994. Trends in caries prevalence in North American children. Int Dent J 44(4 Suppl 1):403-13. Campbell JR, Moss ME, Raubertas RF. 2000.
The association between caries and childhood lead exposure. Environ Health Perspect. 108:1099-102. Canfield RL, Henderson Jr CR, Cory-Slechta DA, Cox C, Jusko TA, Lanphear BP. 2003. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med. 348:1517-26. Capar SG, Gould JH. 1979. Lead, fluoride and other elements in bone meal supplements. J. Assoc. Off. Anal. Chem. 62:1054-1061. Carvalho JC, Van Nieuwenhuysen JP, D’Hoore W. 2001. The decline in dental caries among Belgian children between 1983 and 1998. Community Dentistry and Oral Epidemiology 29 (1):55-61.CDC. Centers for Disease Control and Prevention. 1999. Achievements in public health, 1900–1999: Fluoridation of drinking water to prevent dental caries. Morbid. and Mortal. Weekly Rep. 48(41):933-940. CDC. Centers for Disease Control and Prevention. 2009. Forth national report on human exposure to environmental chemical. http://www.cdc.gov. Cited in Kim 2017. Chen HS, Tsai YC, Chen KK, Tseng YC, Hsu KJ. 2012. Detrimental Effects of Maternal Lead Exposure during Pregnancy and Lactation on Molar Development in the Young Rat. Bulletin of Environmental Contamination and Toxicology89(2):240-244. Colquhoun J. 1993. Fluorides and the decline in tooth decay in New Zealand. Fluoride 26:125-134. Colquhoun J. 1997. Why I changed my mind on water Fluoridation. Perspectives in Biology and Medicine. 41:1-16. Coplan MJ, Masters RD, Hone B. 1999. Silicofluoride Usage, Tooth Decay and Children’s Blood Lead. Poster presentation to Conference on Environmental Influences on Children: Brain, Development and Behavior. New York Academy of Medicine, Mt. Sinai Hospital, New York, May 24-25, 1999.de Liefde B. 1998. The decline of caries in New Zealand over the past 40 years. New Zealand Dental Journal 94(417):109-113.der Fehr FR, Haugejorden O. 1997. The start of caries decline and related fluoride use in Norway. European Journal of Oral Sciences 105(1):21-26.Diesendorf M. 1986. The mystery of declining tooth decay. Nature 322:125-129. Diesendorf M. 1988. International symposium on fluoridation, Social Science and Medicine 27(9):1003-1005. Diesendorf M. 1990. Have the benefits of water fluoridation been over-estimated? Int. Clin. Nut. Rev. 10(2):292-303. Downer MC. 1994. Caries prevalence in the United Kingdom. Int Dent J 44(4 Suppl 1):365-70.Drum K. 2016. Lead: America’s Real Criminal Element. The hidden villain behind violent crime, lower IQs, and even the ADHD epidemic. http://www.motherjones.com/environment/2016/02/lead-exposure-gasoline-crime-increase children-health/Fagin D. 2008. Second Thoughts about Fluoride. New research indicates that a cavity-fighting treatment could berisky if overused. Scientific American January. 74-81.Gemmel A, Tavares M, Alperin S, Soncini J, Daniel D, Dunn J, Crawford S, Braveman N, Clarkson TW, McKinlay S, Bellinger DC. 2002. Blood lead level and dental caries in school-age children. Environmental Health Perspectives110(10):625-630. Gerlach R, de Souza AP, Cury JA, Line SRP. 2000. Effect of lead, cadmium and zinc on the activity of enamel matrixproteinases in vitro. European Journal Of Oral Sciences 108(4):327-34. Gerlach RF, Cury JA, Krug FJ, Line SR. 2002. Effect of lead on dental enamel formation. Toxicology 175:27-34. Gil F, Perez ML, Facio A, Villanueva E, Tojo R, Gil A. 1994. Dental lead levels in the Galician population, Spain. SciTotal Environ 156:145-150.Gil F, Facio A, Villanueva E, Perez ML, Tojo R, Gil A. 1996. The association of tooth lead content with dental health factors. Sci Total Environ 192:183-191. Gillcrist JA. 1996 Fluoridation status of Tennesseans, declining caries prevalence rates, increasing fluorosis, and a review of the appropriate use of fluoride products, The Journal of the Tennessee Dental Association 76(3):12-17. Goyer RA. 1990. Transplacental Transport of Lead. Environmental Health Perspectives. 89:101-105. Goyer RA. 1995. Nutrition and metal toxicity. Am. J. Clin. Nutr. 61(3 Suppl.):646S-650S.Hac E, Czarnowski W, Gos T, Krechniak J. 1997. Lead and fluoride content in human bone and hair in the Gdansk region. Science of the Total Environment 206(2-3):249-254. Haugejorden, O. 1996. Using the DMF gender difference to assess the “major” role of fluoride toothpastes in the caries decline in industrialized countries: a meta-analysis. Community Dentistry and Oral Epidemiology 24(6):369-375.Kalsbeek H, Kwant GW, Groeneveld A, Backer Dirks O, van Eck AAMJ, Theuns HM. 1993. Caries experience of 15-year-old children in the Netherlands after discontinuation of water fluoridation. Caries Res 27:201-5.Kaste LM, Selwitz RH, Oldakowski RJ, Brunelle JA, Winn DM, Brown LJ. 1996. Coronal caries in the primary and permanent dentition of children and adolescents 1–17 years of age: United States, 1988–1991. J Dent Res 75(special issue):631-41.Kato Y, Takimoto S, Ogura H. 1978. Mechanism of induction of hypercalcemia and hyperphosphatemia by lead acetate in the rat. Calcified Tissue Research 24(1):41-6.Kelly JE, Harvey CR. 1979. Basic dental examination findings of persons 1-74 years. In: Basic data on dental examination findings of persons 1-74 years, United States, 1971-1974. Hyattsville, MD: US Department of Health, Education, and Welfare, Public Health Service, Office of Health Research, Statistics, and Technology, National Centre for Health Statistics, DHEW publication no. (PHS) 79-1662. (Vital and health statistics data from the National Health Interview Survey; series 11, no. 214). Kim Y-S, Ha M, Kwon H-J, Kim H-Y, Chou Y-H. 2017. Association between Low blood lead levels and increased risk of dental caries in children: a cross-sectional study BMC Oral Health 17:42.Ko L, Thiessen KM. 2015. A critique of recent economic evaluations of community water fluoridation. International Journal of Occupational and Environmental Health. 21(2):91-120. Koh K, Brook AH. 2014. Environmental stresses affect development: Evidence from dental development in a Romano-British sample. Conference Abstract. KNOHS. Korean National Oral Health Survey. Korean center of disease center. 2012. http://knhanes.cdc.go.kr. Citedin Kim 2017.Krasse B. 1996. The caries decline: is the effect of fluoride toothpaste overrated? European Journal of Oral Sciences,vol. 104(4):426-429. Kristensen LJ. 2015. Quantification of atmospheric Lead emissions from 70 years of leaded petrol consumption in Australia. Atmospheric Environment. 111:195-201.Kumar JV, Swango PA, Linginger LL, Leske GS, Green EL, Haley VB. 1998. Changes in Dental Fluorosis and Dental Caries in Newburgh and Kingston, New York. American Journal of Public Health. 88(12):1866-1870. Künzel W, Fischer T, Lorenz R, Brühmann S. 2000. Decline of caries prevalence after cessation of water fluoridation in the former East Germany. Community Dent Oral Epidemiol. 28:382-9.Lawson BF, Stout FW, Ahern DE, Sneed WD. 1971. The incidence of enamel hypoplasia associated with chronic pediatric lead poisoning. S C Dent J. 29:5-10Leverett DH. 1982. Fluorides and the changing prevalence of dental caries. Science 217, 2 July.Leite GAS, Sawan RMM, Teofilo JM, Porto IM, de Sousa FB, Gerlach R. 2011. Exposure to lead exacerbates dental fluorosis. Archives of Oral Biology 56(7):695-702.Lo GL, Bagramian RA. 1997. Declining prevalence of dental caries in school children in Singapore. Oral Diseases3(2):121-125.Löfgren Å, Hammar H. 2000. The phase-out of leaded gasoline in the EU: a successful failure? Transportation Research Part D: Transport and Environment 5(6, November):419-431.Martin MD, Benton T, Bernardo M, Woods JS, Townes BD, Luis H, et al. 2007. The association of dental caries with blood lead in children when adjusted for IQ and neurobehavioral performance. Sci Total Environ. 377:159-64.Masters RD. 1999. Poisoning the Well: Neurotoxic Metals, Water Treatment and Human Behavior. Plenary address to Annual Conference of the Association for Politics and the Life Sciences, Four Seasons Hotel, Atlanta, GA(September 2, 1999).Milsom KM, Blinkhorn AS, Walsh T, Worthington HV, Kearney-Mitchell P,
Whitehead H, Tickle M. 2011. A Cluster-randomized Controlled Trial: Fluoride Varnish in School Children J Dent Res 90(11).Moss ME, Lanphear BP, Auinger P. 1999. Association of Dental Caries and Blood Lead Levels. JAMA. 281:2294-2298.NCHS. 1974. National Center for Health Statistics. Decayed, Missing, and Filled Teeth Among Youth 12-17 Years -United States. Rockville, Maryland: US Department of Health, Education, and Welfare, Public Health Service, Health Resources Administration Vital and Health Statistics 11(144). DHEW publication no. (HRA)75-1626.Needleman HL, Gunnoe C, Leviton A, et al. 1979. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N Engl J Med. 300:689-695.Nevin R. 2000. How Lead Exposure Relates to Temporal Changes in IQ, Violent Crime, and Unwed Pregnancy. Environmental Research 83(1):1-22.Newbrun E. 2010. What we know and do not know about fluoride. Journal of Public Health Dentistry. 1-7.NIDR. National Institute of Dental Research. 1981. The prevalence of dental caries in United States children, 1979-1980. Bethesda, MD: U.S. Public Health Service, Department of Health and Human Services, National Institutes of Health, NIH publication no. 82-2245.NIDR. National Institute of Dental Research. Oral health of United States children. 1989. The National Survey of Dental Caries in U.S. School Children: 1986–1987. National and regional findings. Bethesda, MD: US Department of Health and Human Services, Public Health Service, National National Institutes of Health, National Institute of Dental Research, NIH publication no. 89-2247.O’Mullane D. 1982. The changing pattern of dental caries in Irish school children between 1961 and 1981. J Dent Res61(Sp Iss):1317-1320.Pain GN. 2015. Plumbosolvency exacerbated by Water Fluoridation.https://www.researchgate.net/publication/282439972_Plumbosolvency_exacerbated_by_Water_FluoridationPetersson GH, Bratthall D. 1996. The caries decline: a review of reviews. European Journal of Oral Sciences 104(4)
Peterson PE. 2003. Fluoride in Drinking Water. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century – The Approach of the WHO Global Oral Health Programme (WHO/NMH/NPH/ORH/03.2).Geneva: WHO Global Oral Health Program. Online at http://www.who.int/oral_health/publications/report03/en/.Pirkle JL, Brody DJ, Gunter EW, Kramer RA, Paschal DC, Flegal KM, Matte TD. 1994. The Decline in Blood Lead Levelsin the United States The National Health and Nutrition Examination Surveys (NHANES). JAMA. 272(4):284-291.Sawan RMM, Leite GAS, Saraiva MCP, Barbosa F Jr, Tanus-Santos JE, Gerlach RF. 2010. Fluoride increases lead concentrations in whole blood and in calcified tissues from lead-exposed rats. Toxicology 271(1-2):21-26.Stewart DJ. 1974. Teeth as indicators of exposure of children to lead. Archives of Disease in Childhood. 49:895.Taylor MP, Winder C, Lanphear BP. 2014. Australia’s leading public health body delays action on the revision of the public health goal for blood lead exposures. Environment International 70:113-117.Vrbic V. 2000. Reasons for the caries decline in Slovenia. Community Dentistry and Oral Epidemiology, vol. 28(2):126-132.Watson GE, Davis BA, Raubertas RF, Pearson SK, Bowen WH. 1997. Influence of maternal lead ingestion on caries in rat pups. Nat Med. 3:1024-1025.WHO. World Health Organization. Global oral health surveillance program. Available online. Wiener RC, Long DL, Jurevic RJ. 2015. Blood levels of the heavy metal, lead, and caries in children aged 24–72 months: NHANES III. Caries Res. 49(1):26-33.Wong MCM, Glenny AM, Tsang BWK, Lo ECM, Worthington HV, Marinho VCC. 2010. Topical fluoride as a cause of dental fluorosis in children (Review). Cochrane Database of Systematic Reviews 2010, Issue 1 Art. No.: CD007693.DOI:10.1002/14651858.CD007693.pub2.Youravong N, Chongsuvivatwong V, Geater AF, Dahlén G, Teanpaisan R. 2006. Lead associated caries development in children living in a lead contaminated area, Thailand. Sci Total Environ. 361:88-96.Ziegelbecker R. 1998. Fluoridation in Europe. Fluoride 31(3):171-1