This boondoggle is full of inaccuracies.
It is well presented but ignores true science. No clever language can change the fact that fluorides
are accumulative, and poisonous toplants,insects, animals,humans anddamage the environment.
This, our modified article is not protected by copyright.
It is in the public domain, please feel free to copy and quote.
Guidelines for Use of Fluorides in Australia: Update 2019
National Oral Health Promotion Clearinghouse, Australian Research Centre for Population Oral Health, The University of Adelaide, Adelaide 2019
Professor Loc Giang Do [Now in Queensland.]
This article has been accepted for publication and undergone full peer review but has not been through the copy editing, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record.
Please cite this article as doi: 10.1111/ADJ.12742
.
ACKNOWLEDGEMENT
National Oral Health Promotion Clearinghouse, Australian Research Centre for Population Oral Health Australian Dental Association Australian Dental and Oral Health Therapists’ Association Dental Hygienists Association of Australia (DHAA Ltd) Colgate Oral Care
J Aldis, J Miller, AJ Spencer, LG Do and D Brennan organised the Workshop. Presenters reviewed and presented evidence of specific topics for discussion. WM Thomson moderated the discussion.
LG Do and AJ Spencer prepared the Guidelines document. Attendees provided feedback and approved the final document.
.
DISCLAIMER
These guidelines reflect the consensus view of the 60 attendees at the workshop, drawn from all states and territories and representing academics from Australian dental schools, jurisdictional health authorities and peak organizations in dentistry. While the guidelines reflect the views of those attending the workshop, they may not reflect the views of the organizations with which those attendees are affiliated.
.
Attendees
(P) denotes presenter at the workshop
Jacqueline Aldis, Sandra Anderson, Peter Arrow (P), Janis Baines (P), Derek Bazen, Linda Bertram-Takacs, David Brennan (P), Bijun Cai, Lyn Carman, Susan Cartwright (P), Mikaela Chinotti, Matthew Hopcraft, Eithne Irving, Lisa Jamieson (P), Kostas Kapellas, Jeroen Kroon, Yvonne Lai, Dianne Lantry, Adrienne Lewis, Liana Luzzi, Stuart Marshall, Angela Masoe, Susanne Sofronoff, Woosung Sohn (P), Youngha Song, A. John Spencer (P), Nicole Stormon, W. Murray Thomson (Moderator), Frederick Wright (P), Sergio Chrisopoulos, Deborah Cole, Cathy Connor (P), Stuart Dashper (P), Yvonne Dimitropoulos, Loc G Do (P), Ian Epondulan, Catherine Feeney, Mario Ferrari, Michael Foley (P), Ashlea Furlan, Diep H Ha (P), Martin Hall, Chris Handbury, Jane Harford (P), Kelly Hennessy, Jenny McKibben, Jennifer Miller, Paula Moynihan, Utz Mueller (P), Rahul Nair, Carol Nevin, Kristy Nixon, Peter Osborne, Mark Penrose, Melissa Plath, Anil Raichur, Sarah Raphael, Kaye Roberts-Thomson (P), Tanya Schinkevitsch, John Skinner and Karen Smart.
.
DR. LOC DO (Orcid ID : 0000-0003-3684-9949)
Article type: Review (by invitation of Editor)
History will be unkind to the above list of compliant attendees. They could be accused of ignorance, dishonest science, or criminal behaviour, or all of the above, only time will tell…
Those promoting this archaic and dangerous protocol reveal their ignorance and incompetence and will bring shame to The University of Adelaide, The Dental Profession, and true science.
.
Australian Research Centre for Population Oral Health, The University of Adelaide, Adelaide 2019
Professor Loc Do [Now in Queensland.]
Running Head: Guidelines for Use of Fluorides in Australia
Abstract:
Fluoride use is the cornerstone of dental caries prevention. [ No longer HERE ] There are numerous sources of fluoride which may have different balance of risks and benefits. The first National Guidelines for Use of Fluorides in Australia were developed at a national Workshop in 2005, and updated in 2012. Since then, more evidence on the balance of risks and benefits of fluoride has become available. A third national Workshop was convened in 2019 to update the Guidelines for Use of Fluorides in Australia.
Poor oral health is a major health issue. Oral conditions affect 3.9 billion people worldwide, with untreated decay in permanent teeth the most prevalent condition globally. Dental caries is the most prevalent oral disease in Australian children and Australian adults. Dental caries has significant negative impact on health, development, behaviours and quality of life of the affected individuals and their surroundings, as well as economic cost on the society consistent with widespread dental problems, dental health expenditure in Australia is large, amounting to $10.15 billion in 2016-17.
We agree that dental health is a major key to general health. The statistics of tooth decay in Australia prove that fluorides in food water and air are a problem – not a solution. Fluoridation is not working.
While sugar consumption and dental plaque remain as key aetiological factors for dental caries, the use of fluorides has been the cornerstone of caries prevention. Research has led to the development of two central preventive programs involving water fluoridation and use of fluoridated toothpaste. Water fluoridation (WF) is recognized as one of the most effective public health interventions. [Your religion not ours.]
The efficacy of fluoridated toothpaste is well established, and while it is an individual behaviour, toothbrushing with a fluoridated toothpaste is widespread across the population.
Development of the national guidelines on fluoride use
In October 2005, ARCPOH hosted a workshop on The Use of Fluorides in Australia, aimed to update information on the nature and distribution of dental caries and fluorosis; to update information on the nature and use (or exposure) to fluorides; to consider the trade-off of the benefit of caries prevention versus the risk of dental fluorosis; to review the evidence of the efficacy/effectiveness of a range of individual fluorides in caries prevention and their risks for creation of dental fluorosis; and to develop guidelines for the use of fluorides in Australia. A second workshop was held in Adelaide in August 2012 to review those guidelines using critical reviews of the latest national and international evidence a total of 10 recommendations from the 2005 workshop remained unchanged as no new evidence was available to warrant amendment, and 6 recommendations were amended.
A third workshop on ‘The use of Fluorides in Australia’ was held in February 2019 in Adelaide, attended by 60 academic and dental health professional experts. The workshop was moderated by Professor Murray Thomson of the University of Otago. In this workshop, presentations were held on the themes of oral disease, effects of fluoridation on dental and human health, and the use of discretionary and professionally applied fluorides. This update of the fluoride guidelines reflects the presentations and consensus discussion from that workshop.
Recent evidence: oral diseases in Australia: dental caries and dental fluorosis
Dental caries in children
Dental caries, the primary target condition of any dental program using fluorides, is one of the most prevalent and important chronic conditions in children. Dental caries is a serious public health in both developing and industrialised countries.
In the 2012-14 National Child Oral Health Survey, over 40% children aged 5-10-years had caries caries in their primary teeth with a mean decayed, missing or filled teeth (dmft) of 1.5. Over a quarter of 5-10-year old children had untreated dental caries in their primary dentition. Just under one-quarter of children aged 6–14 years had experienced caries in their permanent teeth with a mean decayed, missing or filled permanent teeth (DMFT) of 0.5. Further, over one in ten with untreated dental caries in their permanent teeth. Maybe fluoridation is not the answer!
While there has been a substantial improvement in children caries experience across the years since World War II, [in both fluoridated and non-fluoridate nations,] changes in the last two decades have been more subtle. In children, there have been small improvements in dental caries experience in the primary dentition during the 1990s and 2000s. During the same period, dental caries experience in the permanent dentition has improved a little more (Do and Spencer 2016). Many children have no or minimal caries experience, but a small proportion still experience elevated levels of caries. Some 20% of children aged 5–10 years carried over 80% of the total population burden of dental caries in the primary dentition. Likewise, some 17% of children aged 11–14 years carried 80% of the total population burden of dental caries in the permanent dentition (Ha et al. 2016).
There are strong geographical variations in child dental caries experience in Australia. Children in Queensland, mostly non-fluoridated until the late 2000s, and in the Northern Territory, with a high proportion of Indigenous children, consistently had higher prevalence and severity of dental caries than the national averages. [Not true ⇒HERE]
Hence, there is a need to maintain the vastly lowered caries experience for most of the child population, and to intervene among individual or groups of children among with higher prevalence and severity of dental caries to further to further improve child dental health in Australia.
Dental caries in adults
Dental caries affects a large majority of Australian adults related. Some three quarters of young adults aged 15–34 years had caries while almost all adults of older ages had dental caries experience. People aged 15–34 years had on average 4.5 teeth affected by caries, but those but those 55+ years, born before the commencement of fluoride use in Australia had more than 20 teeth affected.
Australia’s approach to the use of fluorides has given primacy to achieving a near maximal reduction in dental caries without an unacceptable level of dental fluorosis. Nearly 90% of Australians live in areas with fluoridated drinking water. In addition, most Australian children and adults brush with a fluoridated toothpaste. Water fluoridation, toothpaste use and other fluoride sources are associated with an increase in the prevalence of any fluorosis. Measures aiming at reducing exposure discretionary fluorides from the early 1990s have resulted in significant reduction in the prevalence and severity of dental fluorosis in both fluoridated and non-fluoridated areas in WA and SA. Very population-based survey in NSW in 2007
.
The National Child Oral Health Study 2012-14 provided the first ever national snapshot of the prevalence and severity of dental fluorosis in Australian children. Any level of fluorosis experience (a Thylstrup and Fejerskov (TF) score of 1+) was found in one in six Australian children. However, just under one per cent of children had more definitive dental fluorosis (having a TF 3+ score). Very few children were observed with moderate to severe dental fluorosis (TF scores of 4 or 5).
Research on the natural history of dental fluorosis and its long-term impact has indicated that very mild to mild fluorosis as observed in Australian children diminished over time (Do et al 2016). Dental fluorosis was not found to have long term negative impacts on oral health-related quality of life.
Recent evidence: Update on Nutrient Reference Values for fluorides
Nutrient Reference Values (NRVs) may be established to represent an estimated average requirement (EAR) or an adequate intake (AI) intended to cover average nutrient requirements and/or an upper level (UL) of intake, above which the risk of adverse effects increases. In 2007 an AI and UL were established for fluoride. In 2017, the National Health and Medical Research Council (NHMRC) revised the UL for fluoride for infants and young children up to 8 years of age
.
Two biomarkers were selected for the evidence review for infants and young children; dental caries and dental fluorosis, as measured by the dmf/DMF index and Dean’s index respectively. Eight critical reports were identified (1997-2010); a database search of 977 papers revealed further information from three studies that met the search criteria (GRADE assessment) referred to the Dean studies in US cities during 1936-42 linking dental health and natural fluoride levels in water supplies. An Expert Working Group concluded there were no better data to use as a basis for establishing fluoride NRVs, as contemporary population studies were confounded by fluoridated toothpastes and/or products containing fluoride.
The AI is based on a mean fluoride intake from the diet (including drinking water with NHMRC Drinking Water Guideline of 1.0 mg F/L) that effectively minimises dental caries. The previous AI (0.05 mg/kg body weight (bw)/day) for infants and children up to 8 years old age group was maintained. A change was made in 2017 in that the AI is not considered applicable to infants aged 0-6 months, as breast feeding is assumed for most infants. A new UL of 0.2 mg/kg bw/day, which minimises dental fluorosis of concern, was based on the 95th percentile of fluoride dietary intake assuming fluoridation of water at 1.9 mg/L. Estimated fluoride intakes from all sources (i.e., diet including water and other beverages, fluoridated toothpaste and/or supplements) in Australia and New Zealand for infants and children up to 8 years old were distributed around the AI but less than this new UL. This supports the continued use of fluorides in Australia including the fluoride level for drinking water and widespread use of low fluoride toothpaste from the age of 18 months and regular toothpaste from 6 years.
The National Guidelines on Fluoride Use 2019
A. Community Water Fluoridation
Community water fluoridation has been the cornerstone of efforts to prevent caries in Australia since the 1970s. This position has been underpinned by population oral health research and reaffirmed across several generations of NHMRC reviews including reviews in 1991 and 2007. Previous iterations of these guidelines have had access to these reviews and contemporary research in arriving at its position on community water fluoridation. This iteration of the guidelines again had access to the most recent NHMRC review and even more recent contemporary research.
Effectiveness of water fluoridation
In 2017 the NHMRC conducted an extensive review of the evidence on the effectiveness and safety in arriving at its position on community water fluoridation. In assessing the evidence on water fluoridation and caries, the York Review and an update conducted by NHMRC in 2007 were used as a background. NHMRC of community water fluoridation then considered the Cochrane Review of the Effectiveness of Water Fluoridation. Some shortcomings of the Cochrane Review were noted. the included evidence to before and after non-randomised controlled studies. This had the effect of limiting the evidence to studies predominantly conducted prior to 1975.
[Once a poison, always a poison.]
NHMRC set about collecting further evidence. Evidence on water fluoridation and dental caries was collected through a review of reviews which included a wider range of study designs and collection of primary studies published after those reviews across the period 2012-15, with an emphasis on Australian research. The 2017 NHMRC Review found consistent evidence that water fluoridation at current Australian levels is associated with decreased prevalence and severity of tooth decay in children and adults.
Research published post 2015 from Australia’s National Child Oral Health Study (NCOHS) 24, 25 and the National Survey of Adult Oral Health (NSAOH) 26 extended evidence available on the effectiveness of water fluoridation in reducing dental caries.
Two recent studies among specific sub-populations also added support to the benefits of community water fluoridation. These were conducted in NSW and in a remote Indigenous communities A,⇔B, ⇔C, in far north Queensland.
.
Safety of water fluoridation
The NHMRC Review searched the post-2006 literature for evidence of possible harmful effects of water fluoridation on human health. There are hundreds of scientific papers on the web in english warning of the dangers from natural occurring fluorides, F. emissions from volcanoes, industrial air pollution and vested interests promoting water fluoridation?
The NHMRC Review concluded that water fluoridation at current Australian levels is not associated with cognitive dysfunction, lowered IQ, cancer, hip fracture and Down syndrome. There was no reliable evidence of an association between water fluoridation at current Australian levels and other human health outcomes.
The evidence reviewed by the UK York Review and the Cochrane Review confirmed the dose – response relationship between fluoride levels occurring naturally in drinking water and dental fluorosis. However, most of the studies behind this association were from countries where the levels of naturally occurring fluoride in water supplies are up to five times greater than levels used in Australia for water fluoridation. There have also been concerns over confounding by exposure to other fluorides and the threshold for dental fluorosis of aesthetic concern. Therefore, other literature, predominantly from Australian studies were also considered by the NHMRC Review. In Australia dental fluorosis has declined over a time when the extent of fluoridation in Australia has expanded. Most of the dental fluorosis in Australia is very mild or mild. Research suggests that this level of dental fluorosis is not of aesthetic concern to affected children and adolescents or their parents. Moderate dental fluorosis is uncommon and severe dental fluorosis is rare in Australia.
The prevalence of fluorosis in Australia was well below that documented in the USA which led to the reduction in the US recommended level of fluoride in drinking water to 0.7 mg F/L in draft form in 2011 and formally in 2015 and formally in 2015. Further, the prevalence of fluorosis of concern in Australia either from an aesthetic perspective alone or from a community perspective on the impact of both caries and fluorosis through ratings of oral health, was low considered for the revision of the Use of Fluorides in Australia guidelines in 2012 and no change was made in the fluoride level in drinking water for fluoridation as practised in Australia. This was rationalised on the basis of Australia’s success in maintaining caries prevention in children while simultaneously reducing the prevalence and severity of dental fluorosis since the early 1990s through a range of measures targeting critical exposures in early childhood from the use of fluoridated toothpaste and other discretionary fluorides .
Impact on social and racial inequalities in childhood caries
The NHMRC Review 2007 noted commentary evidence that water fluoridation reduces the inequalities between socioeconomic groups. However, a lack of high-quality, relevant evidence was also noted. The York review, in England, reported “some evidence that water fluoridation reduces reported “insufficient evidence to determine whether WF results in a change in disparities in caries the inequalities in dental health across social classes in 5–12-year olds.” A Cochrane review reported insufficient evidence to determine whether WF results in a change in disparities in caries insufficient evidence to determine whether WF results in a change in disparities in caries across levels of SES.” The recent NHMRC Review found additional evidence suggesting that WF reduces decay for lower socioeconomic groups and regional areas. However evidence was limited, with studies of low quality.
Race- and income-related inequalities in oral health in Australian children by fluoridation were examined recently using national data. Caries was socially patterned, both by race and income. Water fluoridation was associated with lower caries experience in nearly all race and income stratifications of this population-based study. Indexes of inequality indicated that caries experience was concentrated among lower income groups. Absolute inequalities were consistently lower in fluoridated than non-fluoridated areas. Income-related inequality in caries was also lower in fluoridated than in non-fluoridated areas for both Indigenous and non-Indigenous children.
A secondary analysis of a nation-wide longitudinal birth cohort study of Australian children also contributed evidence of impact of water fluoridation on socioeconomic inequalities in child oral health.
The 2019 Guidelines on water fluoridation
Therefore, the Workshop supported the continuation of water fluoridation at current Australian levels and recommended:
1. Water fluoridation should be continued as an effective, efficient, socially equitable and safe population approach to the prevention of caries in Australia.
Water fluoridation should be extended to as many non-fluoridated areas of Australia as possible, supported by all levels of Government.
The level of fluoride in the water supply should be within the range 0.6–1.1 mg/L.
For people who choose to consume bottled or filtered water containing fluoride, manufacturers should be encouraged to market bottled water containing approximately 1.0 mg/L fluoride and water filters that do not remove fluoride. All bottled water and water filters should be clearly labelled to indicate the concentration of fluoride in water consumed or resulting from the use of such products.
People in non-fluoridated areas should obtain the benefits of fluoride in drinking water by using bottled water with fluoride at approximately 1 mg/L. Note to Recommendation # 3: Individual states and territories have set targets and tolerances for fluoride in their water supplies with all being within the range 0.6–1.1 mg/L.
The use of fluoridated toothpaste by children under the age of 6 years has been the focus of guidelines in Australia since 1993. Two strands of action have been pursued: changed practices by children and their parents in the use of fluoridated toothpaste (age of commencement, amount of toothpaste applied to a brush, the size of the working head of the brush, spitting out toothpaste foam and not rinsing, and not eating or licking toothpaste directly from the toothpaste tube); and the availability and recommended use of a low fluoride children’s toothpaste. The reported behaviour of children in toothbrushing indicates that most brush in line with guidelines, apart from about one third of children commencing brushing with fluoridated toothpaste before the recommended age of 18 months. Market leaders in toothpaste products have also supplied low fluoride children’s toothpaste with appropriate labelling on use, something for which they are commended.
The topic of what the concentration of fluoride should be in children’s toothpaste has been visited several times in Australia. In 2012 further consideration was stimulated by the availability of two
Cochrane systematic reviews of the efficacy of fluoridated toothpaste of different fluoride concentrations in toothpaste. Most evidence was on the immature permanent dentition which is erupting from age 6 years. Only four studies were available on the primary dentition. The effect of low fluoride toothpaste compared to a placebo on the primary dentition was limited to one trial in children 6 to 9 years of age. This age range of participants raises the issue of relevancy. Head-to-head comparisons between active interventions were limited to 3 interventions in children with a primary dentition up to the age of 5 years old with mixed results. Two of these studies reported non- equivocal at the 2012 Workshop. Further evidence has become available after the Workshop and is discussed in Appendix 2, Addendum #1.
Evidence of clinical trials assessed in these Cochrane Reviews was therefore in line with the population level evidence, particularly that from Australian research. This includes the lack of significant change in caries in young children after the introduction of low fluoride children’s toothpaste and other alterations to tooth brushing behaviour in Western Australia and in South Australia
Toothpastes – older adults.
As Australia’s population ages, there is an increasing necessity to ensure that the prevention of the major oral diseases affecting older Australians is evidence-based, relevant and accessible to all. The home use of toothpastes by adult Australians is pervasive, with most older Australians using the standard products available which contain 1–1.45 mg/g fluoride (or 1000–1450 ppm). For older Australians with a high risk of root caries (as well as coronal caries) toothpastes containing up to 5 mg/g fluoride (or 5000 ppm) have been available for use.
The international evidence for adult use of 1.5 mg/g fluoride (or 1500 ppm) toothpaste is supportive of the benefits to adults and older persons, but care should be taken in the interpretation of the effectiveness and efficiency given the variability of populations and the scarcity of dedicated, longitudinal clinical trials specifically controlling for enumerable confounding factors. Evidence for the use of 5 mg/g fluoride (5000 ppm) toothpaste, specifically in populations at high risk is more compelling and could guide good practice in most situations specific to older dentitions at elevated risk of caries. Allied health practitioners, registered or enrolled nurses and indigenous health workers who have been trained and are competent may engage provision of toothbrushing and toothpaste advice to individuals and groups of older Australians.
The 2019 Guidelines on fluoridated toothpaste
From the time that teeth first erupt (about six months of age) to the age of 17 months, children’s teeth should be cleaned by a responsible adult, but not with toothpaste.
For children aged 18 months to five years (inclusive), the teeth should be cleaned twice a day with toothpaste containing 0.5–0.55mg/g fluoride (500–550ppm). Toothpaste should always be used under the supervision of a responsible adult. A small pea-sized amount should be applied to a child-sized soft toothbrush and children should spit out, not swallow, and not rinse. Young children should not be permitted to lick or eat toothpaste. Standard toothpaste is not recommended for children under six years of age unless on the advice of a dental professional or a trained health professional.
For people aged six years or more, the teeth should be cleaned twice a day or more frequently with standard fluoride toothpaste containing 1–1.5mg/g fluoride (1000– 1500ppm). People aged six years or more should spit out, not swallow, and not rinse.
For people who do not consume fluoridated water or who are at elevated risk of developing caries for any other reason, guidelines about toothpaste usage should be varied, as needed, based on dental professional or trained health professional advice. Variations could include more frequent use of fluoridated toothpaste, commencement of toothpaste use at a younger age, or earlier commencement of use of standard toothpaste. This guideline may apply particularly to preschool children at elevated risk of caries.
For teenagers, adults and older adults who are at elevated risk of developing caries, dental professional or trained health professional advice should be sought to determine if they should use toothpaste containing a higher concentration (5 mg/g or 5000 ppm) of fluoride.
C. Self-use fluoride products–fluoride supplements
There has been no updated evidence on the effectiveness and safety of fluoride supplements since the last Workshop.
The 2019 Guidelines on fluoride supplements
11. Fluoride supplements in the form of drops or tablets to be chewed and/or swallowed, should not be used.
D. Self-use fluoride products–fluoride mouth rinses
A minority of mouth rinse products purchased by Australian consumers contain fluoride ion at the recommended concentration of 200–900mg/L for daily and weekly use respectively. Some overseas research has examined daily or weekly supervised fluoride mouth rinse programmes as a strategy for sub-populations such as school children. However, no such programmes are being pursued in Australia. Instead, fluoride mouth rinses offer an additional fluoride vehicle for individuals with elevated risk of caries. Population data reveal that the use of fluoride mouth rinse increases among adolescents (Do and Spencer 2016). This suggests that it may represent an appealing additional source of fluoride among adolescents deemed to be at elevated risk of developing caries. However, it would be important to ensure that any such use of mouth rinse would not substitute for toothbrushing with fluoridated toothpaste. Children aged less than six years should not use fluoride mouth rinses because of the probability of its ingestion and risk of dental fluorosis.
The 2019 Guideline on fluoride mouth rinses
Children below the age of six years should not use fluoride mouth rinse.
Fluoride mouth rinse may be used by people aged six years or more who have an elevated risk of developing caries. Fluoride mouth rinse should be used at a time of day when toothpaste is not used, and it should not be a substitute for brushing with fluoridated toothpaste. After rinsing, mouth rinse should be spat out, not swallowed.
E. Professionally applied fluoride products
Fluoride varnishes
Fluoride varnish contains 22.6mg/ml fluoride ion suspended in an alcohol and resin base. The most common product available in Australia is Duraphat. It is applied by dental and other health professionals directly to dried teeth where it forms a waxy film that adheres to the teeth until it is worn off by chewing or brushing. There are other fluoride-containing varnish products on market today, with varying compositions and delivery systems. However, most are registered for use with dentine hypersensitivity not for the prevention of caries.
Fluoride varnish is effective in reducing caries in young children, adolescents and adults; for the prevention of coronal caries on all surfaces of the teeth; and for the prevention of root caries. Their application up to four times a year has not been linked to an increased risk of dental fluorosis.
There are provisions in place in most Australian jurisdictions for application of topical fluoride varnish by non-dental professionals. This broadens the opportunity for their use. Dental assistants with appropriate training may be involved in applying fluoride varnish. Other non-dental professionals who may be involved are usually registered or enrolled nurses, rural/remote health workers or Aboriginal health workers who have undergone specific training overseen by dental professionals. There is also scope for non-dental professionals use of fluoride varnish to be included in the remit of residential aged care workers and others who work with vulnerable populations.
The 2019 Guideline on fluoride varnishes
14. Fluoride varnish should be used for people who have an elevated risk of developing caries, including children under the age of 10 years.
Fluoride gel and foam
Fluoride gels contain a high concentration of fluoride, typically up to 12.3mg/g fluoride. They are applied by dental professionals using trays that retain the material on the teeth for several minutes. After removal of trays, patients must spit out the residual gel. There is evidence of their effectiveness in children, however, they are contra-indicated for use in children under the age of 10 because large amounts of fluoride can be ingested. Further, fluoride gels appear more efficacious in the permanent dentition. The reviews found no evidence that the effect was dependent on frequency of applications. Like all forms of professionally provided fluoride, gels offer an alternative vehicle for caries prevention for individuals deemed to be at an elevated risk and in whom other fluoride modalities are not available or suitable.
The 2019 Guideline on fluoride gel
15. High concentration fluoride gels (those containing more than 1.5mg/g fluoride ion) may be used for people aged 10 years or more who are at an elevated risk of developing caries.
Silver diamine fluoride
Since its development in the late 1960s silver diamine fluoride (SDF) has been used widely in several countries. The US Food and Drug Administration (FDA) granted its breakthrough therapy designation to silver diamine fluoride 38% for use in arresting dental caries in children and adults in 2016. In Australia, SDF is approved by the Therapeutics Goods Administration (TGA) to treat dentinal hypersensitivity.
Studies have tested SDF, using different concentrations and varying application regimes. There has been a resurgence of interest since its large-scale use, in the form of silver fluoride (SF), in public dental service for children in Australia in the 1980s. The findings to date suggest that the application of 38% SDF twice yearly is effective in arresting active carious lesions in primary teeth and root caries in permanent teeth among the elderly, and its major side effect is the black staining of the carious lesion. SF has been found comparable to atraumatic restorations with GIC in very remote Indigenous children. Its use may be indicated in situations where traditional treatment approaches to caries management may not be possible due to behavioural or medical management challenges, or where access to care is difficult or not available.
The 2019 Guideline on silver diamine fluoride
16. Silver diamine fluoride or silver fluoride may be used for people with caries in situations where traditional treatment approaches to caries management may not be possible.
F. Monitoring and developing caries prevention strategies in the population
The use of fluoride for promoting oral health has always involved a balance between the protective benefit against caries and the risk of developing fluorosis when used in young children. Monitoring fluoride exposure in childhood continues to be important in preserving the effectiveness of fluorides in caries prevention while limiting the risk of fluorosis. Appropriate guidelines that are based on evaluation of risk and benefit of each component of fluoride use can lead to a more beneficial outcome.
There will be a continuing need to review and revise guidelines for the best strategies to prevent dental caries. As noted above in the review of several fluoride vehicles, modifications of the existing guidelines become necessary for reasons including new evidence from clinical trials, changing patterns of behaviour that alter the nature and amount of exposure to fluoride, and emergence of new evidence about the epidemiology of caries and fluorosis. In anticipation of the need for future revisions to these guidelines, it will be important, as in the present instance, to strengthen the evidence-base about individual fluoride vehicles, dental clinical practice, population exposures, and the distribution of oral conditions, particularly the prevalence of caries and fluorosis and the psychosocial impact of both conditions.
Concurrently, it is important to identify and evaluate all preventive strategies, including caries- preventive agents that are not based on fluoride, such as calcium-phosphate caries preventive agents, xylitol and chlorhexidine. Dental professionals, their patients and the community need to be informed about the potential advantages and disadvantages of new interventions, and whether those new interventions should be used in addition to, or as a substitute for, existing preventive interventions. Interventions that appear promising need to be subjected to clinical trials among the target populations in whom they would be intended for use. Any new preventive agents should be adopted only if they are shown to be at least as effective as existing preventive strategies. It is not enough to adopt interventions merely because they appear promising, even if they are known to cause no harm, because their use may forego opportunities to provide other care that is effective. After the adoption of efficacious interventions in clinical practice or public health settings, their community effectiveness should be monitored through population-based studies.
Therefore,
17. ) There is a need to support further studies that examine the impact of fluoride vehicles in the Australian population including: studies of the epidemiology of dental caries and dental fluorosis; investigations of the impact of both conditions on people’s well-being and quality of life; risk factors for dental caries and dental fluorosis; use of fluoride vehicles in dental practice and the population; and the efficacy, effectiveness and cost effectiveness of fluoride vehicles.
18.) Research is needed to develop new preventive interventions including new vehicles for fluoride delivery as well as other preventive strategies that are not based on fluoride. New interventions should be judged for their equivalency or superiority to existing preventive approaches that have documented efficacy.
Note to Recommendation # 18: Further discussion is provided in Appendix 2, Addendum # 2. Note: All Recommendations are listed in Appendix 1.
ACKNOWLEDGEMENT
National Oral Health Promotion Clearinghouse, Australian Research Centre for Population Oral Health Australian Dental Association Australian Dental and Oral Health Therapists’ Association Dental Hygienists Association of Australia (DHAA Ltd) Colgate Oral Care
J Aldis, J Miller, AJ Spencer, LG Do and D Brennan organised the Workshop. Presenters reviewed and presented evidence of specific topics for discussion. WM Thomson moderated the discussion.
LG Do and AJ Spencer prepared the Guidelines document. Attendees provided feedback and approved the final document.
DISCLAIMER
These guidelines reflect the consensus [Note: not unanimous] view of the 60 attendees at the workshop, drawn from all states and territories and representing academics from Australian dental schools, jurisdictional health authorities and peak organizations in dentistry. While the guidelines reflect the views of those attending the workshop, they may not reflect the views of the organizations with which those attendees are affiliated.
Attendees
(P) denotes presenter at the workshop
Jacqueline Aldis Sandra Anderson Peter Arrow (P) Janis Baines (P) Derek Bazen Linda Bertram-Takacs David Brennan (P) Bijun Cai
Lyn Carman Susan Cartwright (P)
Matthew Hopcraft Eithne Irving Lisa Jamieson (P) Kostas Kapellas Jeroen Kroon Yvonne Lai Dianne Lantry Adrienne Lewis Liana Luzzi
Stuart Marshall
Susanne Sofronoff Woosung Sohn (P) Youngha Song A. John Spencer (P) Nicole Stormon
W. Murray Thomson (Moderator)
Frederick Wright (P)
Mikaela Chinotti Sergio Chrisopoulos Deborah Cole Cathy Connor (P) Stuart Dashper (P) Yvonne Dimitropoulos Loc G Do (P)
Ian Epondulan Catherine Feeney Mario Ferrari Michael Foley (P) Ashlea Furlan Diep H Ha (P) Martin Hall
Chris Handbury Jane Harford (P) Kelly Hennessy
Angela Masoe Jenny McKibben Jennifer Miller Paula Moynihan Utz Mueller (P) Rahul Nair
Carol Nevin Kristy Nixon Peter Osborne Mark Penrose Melissa Plath Anil Raichur Sarah Raphael Kaye Roberts-Thomson (P)
Tanya Schinkevitsch John Skinner
Karen Smart
References
Marcenes W, Kassebaum NJ, Bernabe E, Flaxman A, Naghavi M, Lopez A, Murray CJ. Global burden of oral conditions in 1990-2010: a systematic analysis. J Dent Res. 2013; 92:592-597.
Do L and Spencer A. Oral health of Australian children. The National Child Oral Health Study 2012-14. 2016, Adelaide: University Press.
Slade G, Spencer A, Roberts-Thomson K. Australia’s dental generations: the National Survey of Adult Oral Health 2004-06. Vol. AIHW cat. no. DEN 165. 2007, Canberra: Australian Institute of Health and Welfare.
Casamassimo PS, Thikkurissy S, Edelstein BL, Maiorini E. Beyond the dmft: the human and economic cost of early childhood caries. J Am Dent Assoc. 2009; 140:650-657.
AIHW. Health expenditure Australia 2016–17. in Health and welfare expenditure series no. 64. Cat. no. HWE 74. 2018, Australian Institute of Health and Welfare Canberra.
McDonagh MS, Whiting PF, Wilson PM, Sutton AJ, Chestnutt I, Cooper J, Misso K, Bradley M, Treasure E, Kleijnen J. Systematic review of water fluoridation. BMJ. 2000; 321:855-859.
NHMRC. Review of water fluoridation and fluoride intake from discretionary fluoride supplements. 1999, National Health and Research Council: Melbourne.
CDC. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States. 2001, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta.
ARCPOH. The use of fluorides in Australia: guidelines. Aust Dent J. 2006; 51:195-199.
ARCPOH. Fluoride Review Guidelines 2012. 2014, Australian Research Centre forPopulation Oral Health: Adelaide.
Ha DH, Roberts-Thomson KF, Peres KG, Arrow P, Do LG. Oral health status of Australian children. in Oral health of Australian children: the National Child Oral Health Survey 2012–14, Do L G, et al., Editors. 2016, University Press: Adelaide.
Do LG and Spencer AJ. Risk-benefit balance in the use of fluoride among youngchildren. J Dent Res. 2007; 86:723-728.
Fejerskov O, Manji F, Baelum V. Dental fluorosis: a handbook for health workers. 1988, Copenhagen: Munksgaard. 123.
Levy SM. An update on fluorides and fluorosis. J Can Dent Assoc. 2003; 69:286-91.
NHMRC. Information paper – Water fluoridation: dental and other human health outcomes. 2017, National Health and Medical Research Council: Canberra.
Riordan PJ. Dental fluorosis decline after changes to supplement and toothpasteregimens. Community Dent Oral Epidemiol. 2002; 30:233-40.
Do LG and Spencer AJ. Decline in the prevalence of dental fluorosis among SouthAustralian children. Community Dent Oral Epidemiol. 2007; 35:282-291.
Do LG, Miller J, Phelan C, Sivaneswaran S, Spencer AJ, Wright C. Dental caries andfluorosis experience of 8-12-year-old children by early-life exposure to fluoride. Community Dent Oral Epidemiol. 2014; 42:553-562.
NRV. Australian and New Zealand Nutrient Reference Values for Fluoride. A report prepared for the Australian Government Department of Health and the New Zealand Ministry of Health. 2017, The Australian Government Department of Health and the New Zealand Ministry of Health: Canberra.
Spencer AJ, Do LG, Mueller U, Baines J, Foley M, Peres MA. Understanding Optimum Fluoride Intake from Population-Level Evidence. Adv Dent Res. 2018; 29:144-156.
NHMRC. A systematic review of the efficacy and safety of fluoridation. 2007, National Health and Research Council: Canberra.
Iheozor-Ejiofor Z, Worthington HV, Walsh T, O’Malley L, Clarkson JE, Macey R, Alam R, Tugwell P, Welch V, Glenny AM. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev. 2015:CD010856.
Rugg-Gunn AJ, Spencer AJ, Whelton HP, Jones C, Beal JF, Castle P, Cooney PV, Johnson J, Kelly MP, Lennon MA, McGinley J, O’Mullane D, Sgan-Cohen HD, Sharma PP, Thomson WM, Woodward SM, Zusman SP. Critique of the review of ‘Water fluoridation for the prevention of dental caries’ published by the Cochrane Collaboration in 2015. Br Dent J. 2016; 220:335-340.
Ha DH, Spencer AJ, Peres KG, Rugg-Gunn AJ, Scott JA, Do LG. Fluoridated Water Modifies the Effect of Breastfeeding on Dental Caries. J Dent Res. 2019; 98:755-762.
Spencer AJ, Do LG, Ha DH. Contemporary evidence on the effectiveness of water fluoridation in the prevention of childhood caries. Community Dent Oral Epidemiol. 2018; 46:407-415.
Do L, Ha D, Peres MA, Skinner J, Byun R, Spencer AJ. Effectiveness of water fluoridation in the prevention of dental caries across adult age groups. Community Dent Oral Epidemiol. 2017; 45:225-232.
Blinkhorn AS, Byun R, Mehta P, Kay M. A 4-year assessment of a new water- fluoridation scheme in New South Wales, Australia. Int Dent J. 2015; 65:156-63.
Kroon J, Lalloo R, Tadakamadla SK, Johnson NW. Dental caries experience in children of a remote Australian Indigenous community following passive and active preventive interventions. Community Dent Oral Epidemiol. 2019; 47:470-476.
HHS. Proposed HHS recommendation for fluoride concentration in drinking water for the prevention of dental caries. The Federal Register, 01/13/2011. 2011, US Department of Health and Human Services. : https://www.federalregister.gov/articles/2011/01/13/2011-637 accessed on 8/12/2013.
HHS. U.S. Public Health Service Recommendation for Fluoride Concentration in Drinking Water for the Prevention of Dental Caries. Public Health Reports. 2015; 130:318-331.
Do LG, Ha DH, Spencer AJ. Natural history and long-term impact of dental fluorosis: a prospective cohort study. Med J Aust. 2016; 204:25.
Spencer AJ and Do LG. Changing risk factors for fluorosis among South Australian children. Community Dent Oral Epidemiol. 2008; 36:210-8.
Do LG, Ha DH, Roberts-Thomson KF, Jamieson L, Peres MA, Spencer AJ. Race- and Income-Related Inequalities in Oral Health in Australian Children by Fluoridation Status. JDR Clin Trans Res. 2018; 3:170-179.
Goldfeld S, Francis KL, Hoq M, Do L, O’Connor E, Mensah F. The Impact of Policy Modifiable Factors on Inequalities in Rates of Child Dental Caries in Australia. Int J Environ Res Public Health. 2019; 16.
Marinho VC. Cochrane reviews of randomized trials of fluoride therapies for preventing dental caries. Eur Arch Paediatr Dent. 2009; 10:183-191.
Walsh T, Worthington HV, Glenny AM, Appelbe P, Marinho VC, Shi X. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2010:Cd007868.
Walsh T, Worthington HV, Glenny AM, Marinho VC, Jeroncic A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019; 3:Cd007868.
Ekstrand KR. High Fluoride Dentifrices for Elderly and Vulnerable Adults: Does It Work and if So, Then Why? Caries Res. 2016; 50 Suppl 1:15-21.
Ekstrand KR, Poulsen JE, Hede B, Twetman S, Qvist V, Ellwood RP. A randomized clinical trial of the anti-caries efficacy of 5,000 compared to 1,450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res. 2013; 47:391-398.
Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013:Cd002279.
Garcia RI, Gregorich SE, Ramos-Gomez F, Braun PA, Wilson A, Albino J, Tiwari T, Harper M, Batliner TS, Rasmussen M, Cheng NF, Santo W, Geltman PL, Henshaw M, Gansky SA. Absence of Fluoride Varnish-Related Adverse Events in Caries Prevention Trials in Young Children, United States. Prev Chronic Dis. 2017; 14:E17.
Tellez M and Wolff MS. The Public Health Reach of High Fluoride Vehicles: Examples of Innovative Approaches. Caries Res. 2016; 50 Suppl 1:61-67.
Marinho VC, Worthington HV, Walsh T, Chong LY. Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2015:Cd002280.
Twetman S and Keller MK. Fluoride Rinses, Gels and Foams: An Update of Controlled Clinical Trials. Caries Res. 2016; 50 Suppl 1:38-44.
Weyant RJ, Tracy SL, Anselmo TT, Beltran-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013; 144:1279-91.
Rosenblatt A, Stamford TC, Niederman R. Silver diamine fluoride: a caries “silver- fluoride bullet”. J Dent Res. 2009; 88:116-125.
Horst JA. Silver Fluoride as a Treatment for Dental Caries. Adv Dent Res. 2018; 29:135-140.
Roberts-Thomson KF, Ha DH, Wooley S, Meihubers S, Do LG. Community trial of silver fluoride treatment for deciduous dentition caries in remote Indigenous communities.
Aust Dent J. 2019; 64:175-180.
We are surprised that the paper makes no mention of lead as a major cause of dental decay!
https://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.png00yarycoldhttps://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.pngyarycold2020-04-18 10:29:422020-04-18 10:29:42Guidelines for Use of Fluorides in Australia 2019 +
We are told by the Queensland Government, that no adverse effects have been seen in Townsville from fluoridation, but Queensland Health has never provided any health studies to justify this claim!
‘THE EFFECT ON CARIES EXPERIENCE OF LIFETIME RESIDENTS’
A Survey by W. Vidoroni, G.S. Sternberg and G.N. Davies Division of Dental Services, Department of Health, Brisbane, Queensland, Australia, and Dental School, University of Queensland, Turbot St, Brisbane, Australia.
Our criticisms:
Extract
❝ …Another feature of Townsville is the mobility of the population. This is reflected by the fact that although 900 children were examined only 317 or 35 per cent could be classified as lifetime residents, due to large RAAF Base. Data on the remaining non-lifetime residents will be reported in a separate paper. ❞
SoWhere Is It ?
This additional data was promised in the report, but despite numerous telephone requests to one of the authors of this report at the time – W. Videroni, none was ever provided.
More criticisms:
Extract
❝…In addition to assessing the dental caries experience of the children, data was collected on the following:
fluorosis, idiopathic enamel opacities, enamel hypoplasia, tetracycline staining, traumatic injuries to teeth, oral mucosal disease, pathology of bone, dentofacial anomalies, periodontal status (soft deposits, calculus, intense gingivitis), need for periodontal treatment, prosthetic status, denture requirements, conditions needing immediate attention and fillings and extractions required for individual teeth. These data will be reported in a subsequent publication. ❞.
So Where Is It ?
This additional data was promised in the report, but despite numerous telephone requests to one of the authors of this report at the time – W. Videroni – none was ever provided.
Were the RAAF & Lavarack Barracks Base transient residents included?
More Comments:
• Lost in this long list fluoridation negative outcomes, is one of major concern,Dental Fluorosis:
• Dental fluorosis is not reversible and in more severe cases, causes disfigurement, pitting, staining and positional defects.
As can been seen from the newspaper cutting below, Fluoridation of Townsville’s water supply has not had the expected results:
CHILDREN will no longer receive free dental care at school.
The Queensland Government has stopped offering treatment in its school dental vans because there is not enough staff to man them.A letter sent out through schools this week says the vans would only examine students and provide a report to parents on the state of their teeth.They will then have to seek treatment at private dental practices or take their chances with long public dental waiting lists.“Due to expected demand for treatment you may have to wait for a while for an appointment for non-urgent treatment,” the letter said.Queensland Parents and Citizens Association Northern Region president Mick Cutler said parents wanted to see the dental van visits saved.“We would be disappointed but we also understand the reality of change,” Mr Cutler said.“We’d hope they have the capacity to recruit more staff.“When Queensland children have the highest rate of tooth decay in Australia of course we would like to see the dental vans continue.“We also need to continue the education of our children on better eating habits that don’t contribute to (poor dental health).”In the past all Queensland children from four years old to year 10 at school have been eligible for public sector oral health services.The non-emergency dental treatment is provided at schools through dental clinics and dental vans on a rotational basis.Parents sign a consent form allowing the dentists to check for cavities and put in fillings, if necessary.In February 2006 the Townsville Bulletin reported annual free dental check-ups for students across the twin cities would be stretched out to every two years.At the time a health spokeswoman blamed the wait on the twin cities’ population surge.Leading dental researcher Dr Kerrod Hallett said he had been shocked by the sorry state of Townsville tots’ teeth on his last visit to the city.Dr Hallett is trialling a new mouth guard, designed to stop tooth decay, at Vincent State School.The paediatric dentist hopes the trial will stop young children from suffering the pain of tooth aches and rotting teeth.“I examined 16 children on the first day,” he said.“Out of those one had a healthy mouth.“I was quite shocked myself.”Caption: BRUSHED . . . children such as Annabella Schmid, 4, will no longer receive treatment through school dental vans.
~ UPDATE NOVEMBER 2010 ~ Townsville has been fluoridated for 40 + years by the Townsville Council.
… Earlier this year [2012] we asked Townsville Council if they knew of any general health studies that had been done in Townsville for water fluoridation the then Mayor and Director’s representative replied:
❝Townsville Council …. not aware of any specific studies (fluoridation health studies) not commissioned any – not aware of any …. contact Qld. Health to see if they have done any …❞
We are told by the Queensland Government that no adverse effects have been seen in Townsville from fluoridation, but Queensland Health has never provided any health studies to justify this claim – the reason why – they have never looked at anything but teeth. Fluoride, when ingested travels throughout the body in the blood plasma, but supposedly it only beneficially affects teeth? If you don’t look – you don’t find — Just keep on parroting fluoridation is “safe and effective”!
THE NUCLEAR INDUSTRY IS WELL INFORMED AND EXPERIENCED ABOUT FLUORIDES AND CORROSION
Fluoride increases the electrical conductivity of water. In general, the higher the electrical conductivity of water, the higher its ability to allow corrosion to occur to metals it contacts.
Your car, hot water system, house plumbing and mercury teeth fillingswill all be subject to more rust and or corrosion in a
fluoride environment. Aquarium fish, pet dogs, cats, birds, children and some garden plants will also suffer damage …
→Oak Ridge World War 11 Secret City←A city born of war in 1942, existed for seven years as a truly “Secret City.” Oak Ridge, Tennessee was not shown on any maps, did not allow any visitors other than by special approval, had guards posted at the entrances to the city and required all residents to wear badges at all times when outside their homes.
Oak Ridge, Tennessee was born as a direct result of the letter written by Albert Einstein to then President Roosevelt in 1939 citing the urgent need to develop the capability to sustain a chain reaction of uranium. From this letter came the plan for our nation to create an atomic weapon that would be more powerful than any weapon in the history of the world. The Manhattan Project, created to develop this amazing new atomic weapon, spent 60 cents of every dollar in Oak Ridge!
The “Secret City” grew to a population of 75,000, was the fifth largest city in Tennessee and was not even on the map.
~~~~~~◊~~~~~~
The Nuclear Industries Research Demonstrates That Fluorides Are Corrosive. ⇓ ⇓ ⇓
https://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.png00yarycoldhttps://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.pngyarycold2014-09-11 14:33:412014-09-11 14:33:41FLUORIDE-Corrosion – Oak Ridge National Laboratory…
At least 30 days prior to actually ceasing fluoridation, the water supplier must notify Queensland Health and again publish a notice at least once in a newspaper circulating in the area service by the water supply indicating the date it intends to cease fluoridation.
DECOMMISSIONING FLUORIDATION PLANTS – Qld.
Q – Can a local government elect to cease fluoridating communities that are currently fluoridated?
A – Yes
Q – What is the process?
A – Prior to ceasing fluoridation of a water supply that is currently
fluoridated the local government must have made a determination
that ceasing fluoridation is in the best interests of the community.
Once a decision has been made the local government must notify Queensland Health and publish a notice detailing the nature of the decision at least once in a newspaper circulating in the area serviced by the water supply to which the decision relates.
If the local government is not the water supplier for the community the water supplier must be informed of the decision and is bound by the Act to comply with it.
At least 30 days prior to actually ceasing fluoridation, the water supplier must notify Queensland Health and again publish a notice at least once in a newspaper circulating in the area service by the water supply indicating the date it intends to cease fluoridation.
Q –If a non-SEQ local government chooses to cease dosing in certain communities, what costs incurred to date will be reimbursable?
A – The majority of water suppliers outside south east Queensland that are currently dosing would have signed financial agreements under the Queensland Fluoridation Capital Assistance Program (QFCAP) administered by with the Department of State Development, Infrastructure and Planning (DSDIP) to cover up to 100% of costs associated with the installation of fluoride dosing infrastructure. Where there are still claims outstanding under this program these may be submitted to DSDIP even if it is the local government’s decision to cease operation of the relevant infrastructure.
All QFCAP claims must be finalised prior to 30 June 2014 when this funding expires.
Costs that are not reimbursable include:
– costs associated with making the decision to cease fluoridation, including costs associated with compensation to other local governments or the water supplier
– costs associated with the safe decommissioning of fluoride dosing infrastructure
– costs associated with the operation and maintenance of fluoride dosing infrastructure including chemicals, power, operator wages and laboratory testing.
Q – What do we do with plant, equipment and consumables?
A – Where a decision to cease fluoridation is made under the Act the water supplier should ensure that the fluoride dosing facility is fully decommissioned and any remaining fluoride chemicals are 2
disposed of, or removed from site, in compliance with legislative requirements pertaining to those particular chemicals.
Decommissioning should include the physical removal of the fluoride injection point, not just turning off the valve.
Schemes yet to commence fluoridating
Q – Will costs incurred in scoping to date be reimbursed if a local government determines it is not in the best interests of a community to proceed with fluoridation?
A – Yes costs incurred in preparation for the installation of fluoride dosing infrastructure (concept design and tender related costs etc.) incurred in good faith will be reimbursed via the Queensland Fluoridation Capital Assistance Program administered by the Department of State Development, Infrastructure and Planning.
The guidelines around reimbursements of costs where local governments choose not to fluoridate are currently being developed.
Costs associated with the making of the decision not to implement fluoridation cannot be claimed.
Q – If a Local Government is part way through implementation and determines it will not implement fluoridation will the cost of contract penalties be covered?
A – The Department of State Development, Infrastructure and Planning is still considering this matter but the maximum amount available for reimbursement will not exceed the approved funding amount stated in the Financial Incentive Agreement.
Q – If a local government elects to continue and implement fluoridation, will all eligible costs be met?
A – All local governments deciding to proceed with implementation of fluoridation will be able to claim up to 100% funding for the lowest cost option for the installation of fluoride dosing infrastructure. This funding is available from the Queensland Fluoridation Capital Assistance Program administered by the Department of State Development, Infrastructure and Planning.
All funding claims made under this program must be finalised by 30 June 2014.
The water supplier must operate the plant in accordance with the requirements of the Water Fluoridation Act, Regulation and Code of Practice. The supplier must meet all ongoing operation and maintenance costs.
Q – Will an operating cost support fund be established to support smaller local governments?
A – At present the government has not announced any financial assistance for ongoing operation and maintenance costs associated with fluoride dosing infrastructure. 3
Q – Will there be an opportunity in future for capital support costs if a local government decides to proceed with fluoridation?
A – The Queensland Fluoridation Capital Assistance Program administered by the Department of State Development, Infrastructure and Planning currently provides up to 100% funding for the costs associated with the installation of fluoride dosing infrastructure.
This funding expires on 30 June 2014. At present there are no arrangements in place to assist local governments in meeting the costs of fluoride dosing infrastructure beyond this date.
SEQ and schemes where the Local Government is not the water supplier
Q – Where the local government is not the water supplier, who makes the decision about whether fluoridation is in the best interests of the community?
A – The decision as to whether fluoridation is in the best interests of the community is always to be made by the local government.
Where the local government is not the water supplier the Act gives provision for the local government to consult with the water supplier about the cost implications, infrastructure arrangements and potential impact on other water supplies before making a decision as to whether fluoridation is in the best interests of a community.
Q – Where the local government is not the water supplier does the water supplier have to act on the decision to implement or cease fluoridation for a community?
A – Yes, the Act states that the water supplier must comply with the decision made by the local government.
Q – Where the local government is not the water supplier and there are costs to the water supplier associated with implementing or ceasing fluoridation in line with a local government decision, who pays?
A – If a water supplier incurs costs in complying with the decision of a local government to implement or cease fluoridation the Act requires the local government to meet these costs.
Q – If an SEQ local government considers the interests of their communities are best served by discontinuing the supply of fluoridated water, how can they achieve this?
A – The scenarios below provide some guidance on this point:
For communities served by Water Grid-connected water supply infrastructure, if all local governments in SEQ jointly make the decision to cease fluoridation of the drinking water that is supplied to them (or to their jointly owned Distributor/Retailers) by Seqwater, then Seqwater would have to cease fluoridation at all of their water treatment plants.
If only some local governments decided that the supply of fluoridated water to some part or all of their local government area should cease, but others wanted to continue fluoridation, then the obligation would lie with those local governments intending to discontinue fluoridation to implement this decision by negotiation with Seqwater and, potentially, the other impacted local governments. The negotiations would have to address measures to ensure there was no adverse impact on the water supply arrangements for other local governments in the SEQ region. All costs faced by Seqwater or the other impacted local governments, would be the responsibility of the local government or governments that took the decision to cease fluoridation.
A number of Seqwater-owned water treatment plants are not Grid-connected, and serve only one local government area. In these cases, if the relevant local government whose community or communities are served by the Seqwater treatment plant in question decides to discontinue water fluoridation, then Seqwater would have to cease adding fluoride to the relevant water supply.
Best interests of the community
Q – How does a local government determine whether fluoridation is in the best interests of the community?
A – Queensland Health will not direct a local government as to how they determine what is in the best interests of their communities. However, local governments should note that the State Government continues to advocate for the inclusion of fluoride in drinking water.
Fluoridation has been proven as a safe and effective means of preventing tooth decay, for people of all ages and not just for children, and is supported by peak health bodies including the National Health and Medical Research Council, the Australia Dental Association, the Australian Medical Association and the World Health Organization.
When considering whether fluoridation is in the best interests of a community Queensland Health urges local governments to consider the significant oral health benefits that are associated with drinking water fluoridation. With the State Government covering up to 100% of the costs associated with the installation of fluoride dosing infrastructure, local governments should carefully balance the costs to rate payers of operating and maintaining fluoride dosing infrastructure against the cost to rate payers of dental visits associated with tooth decay.
Local governments are urged to ensure they consider their community as whole and not just the opinions of vocal anti-fluoride campaigners. Local governments should note that until the recent changes in the fluoride legislation those who are pro-fluoride have had no reason to voice their support and will not be well-versed in campaigning methods. Councillors should note that an LGAQ survey in 2005 showed that nearly 60% of Queenslanders surveyed favoured fluoridation, while only 21% were opposed to fluoridation. The Government believes that this strong community support for fluoridation should be considered and not just the views of a noisy minority.
Q – How can a local government dispel myths associated with fluoridation and get more information on the health benefits of fluoridation?
A – Queensland Health is able to offer the services of oral health professionals to brief local government representatives on the health benefits of fluoridation and to assist Councillors to determine the credibility of common pro- and anti-fluoridation arguments. 5
To arrange a briefing, please contact Dr Greg Jackson, Director – Water Program, Queensland Health via (07) 332 89345.
Miscellaneous questions
Q – Are exemption applications granted or made under the old version of the Act valid?
A – Any exemption given or exemption application made under the old version of the Act has no effect as fluoridation is no longer mandatory.
Q – Will the State indemnify a local government against all costs and expenses properly incurred, and not recovered, by it in relation to any proceeding taken against the local government as result of making a fluoridation decision.
A – Yes. Local governments have been added to s96 of the Water Fluoridation Act which deals with the provision of indemnity.
Q – What requirements does a water supplier have to comply with if they decide to continue or proceed with the implementation of fluoridation?
A – These have not changed with the recent amendments to the Act. A water supplier adding fluoride to a public potable water supply must comply with the requirements of the Water Fluoridation Act 2008, Water Fluoridation Regulation 2008 and Queensland Water Fluoridation Code of Practice.
Q – Can fluoride tablets be provided as an alternative to water fluoridation?
A – Fluoride supplements, such as tablets and drops, do not provide the same benefit as water fluoridation for several reasons:
They are most likely to be used by the people who need them least – children with good oral hygiene and healthy diets
People who brush their teeth regularly with fluoridated toothpaste receive little, if any, additional benefit from fluoride tablets when sucked or swallowed once a day
People may not remember to take them, or may take too many
They increase the risk of dental fluorosis, without clear benefits
Animal experiments have shown that fluoride given once a day is more likely to cause fluorosis than the same amount of fluoride given intermittently throughout the day, as occurs with fluoridated water.
Since 2006, the Australian Research Centre for Population Oral Health has recommended that fluoride supplements should not be used. Therefore, since 2006, fluoride supplements have been progressively phased out nation-wide.
The Queensland Government does NOT support the use of fluoride tablets.
“Opponents of the fluoridation project were quickly labeled by the masterminds of Alcoa’s PR group as loonies and right-wing extremists who saw fluoridation as a communist plot.
Officials who loudly promote fluoridation of public water claim as their motivation the prevention of dental cavities. They frequently cite studies comparing tooth decay rates in fluoridated areas to unfluoridated areas, which purport to show dramatic reductions in tooth decay in children-as much as a 60 percent difference. If this were true, and fluoride were indeed safe, it would be a truly miraculous substance, but this still would not justify putting it in the water supply because we are being medicated and have not even been given a choice in the matter, as you will see. As it stands, there is in fact no credible evidence that fluoride added to the water supply reduces cavity rates at all, and several studies have convincingly demonstrated that the incidence of cavities is actually higher in fluoridated areas.
Shortly after the turn of the century it was noticed that children in certain areas of the country had a high incidence of damaged teeth. Further investigation disclosed that this mottling of their tooth enamel, now known as “dental fluorosis,” was caused by elevated contents of naturally occurring fluoride in certain water systems. This finding motivated the American Dental Society and the U.S. Public Health Department to call for the removal of fluoride in the water from these areas. H. Trendley Dean of the U.S. Public Heath Department in 1930 conducted the original work on this problem.
At this juncture, Dr. Gerald Cox took up the banner and suggested that using a smaller dose of fluoride could not only prevent dental fluorosis, but could even prevent cavities. He suggested adding 1 ppm of fluoride to the public drinking water. He made this proclamation without any studies, human or otherwise, to suggest that it would be effective or safe. What makes this so interesting is that Dr. Cox was on the staff of the Mellon Institute, and the Mellon family owned the Aluminum Company of America (Alcoa). One of the major waste products produced in the aluminum industry is fluoride. Because of its intense corrosive ability and extreme toxicity, disposal of fluoride had, up until that time, been a very expensive and controversial proposition. So what could the aluminum industry do with all of this toxic fluoride? After all, safe disposal cost the company millions of dollars every year.
Ironically, the answer was to come from government. Fortunately for Alcoa, Andrew Mellon, its founder, was also the Treasury Secretary. Interestingly, the U.S. Public Health Service at that time was under the direct control of the Treasury Secretary. Dr. Dean, who eventually came to support adding 1 ppm fluoride to public water supplies as a safe and effective way to reduce dental caries, became known as “Mr. Fluoridation,” and was chosen by the USPHS to head up the fluoridation studies. As Dr. John Yiamouyiannis noted in his excellent book, Fluoride. The Aging Factor, the American Medical Association (AMA), on September 18, 1943, (as fluoridation was first being proposed) cautioned that fluoride was a powerful protoplasmic poison, and because of its widespread presence in nature, toxic accumulation could be a major problem if water was fluoridated. On October 1, 1944, the Journal of the American Dental Association also noted that: “the potential for harm outweighed those for good.” It would behoove the Association’s present membership to remember that in this same article the ADA recognized that as little as 1.2-3.0 ppm of fluoride in drinking water was associated with “developmental disturbances in bones as osteosclerosis, spondylosis and osteoporosis, as well as goiter.”
Despite these cautionary warnings, Dr. Cox convinced Dr. J.J. Frisch, a Wisconsin dentist, to actively promote fluoridation of the water supply. According to historians of the era, Frisch led the charge with the frenzy of a religious zealot and turned it into a political crusade. These developments were, of course, just what Alcoa’s owners wanted. In 1944, according to Hearings before the Committee on Interstate and Foreign Commerce held on May 25-27, 1954. Alcoa hired a powerful attorney, Oscar Ewing, and paid him an annual salary of $750,000, even though Alcoa wasn’t facing any major litigation. A few months after being hired, he left the company to accept a job as Federal Security Administrator, a position that put him in charge of the USPHS and under the direct control of, – you guessed it, Treasury Secretary Mellon. It should also be noted that he made a great deal of fanfare about leaving such a well-paid job to serve his country. Not surprisingly, Ewing launched a vigorous nationwide campaign to promote fluoridation of public water supplies.
The fluoridation effort was no small project, and certainly not one that Ewing intended to lose. He hired the best public relations master money could buy: Edward L. Bernays, labeled by The Washington Post as “the original spin doctor.” In addition to his other credentials, Bernays was also the nephew of Sigmund Freud. Bernays knew the best route to take was to get the endorsement of the dental and medical professionals, since the public depended on their wisdom in these matters, and generally trusted them. By using all of the powers at their command Mellon’s fluoridation team convinced the city council of Grand Rapids, Michigan, to allow its water supply to be fluoridated, with the city of Muskegon serving as an unfluoridated control in the experiment. The project was to begin on January 25, 1945, and would be the first U.S. city to add fluoride to its drinking water.
Two things need to be understood at this point. First, the recommendation was accepted just three months after the dire warnings expressed by both the AMA and the ADA. Second, even at that time there was significant evidence that fluoride was toxic to cells in small concentrations, yet these devious men proceeded despite the fact that no human studies had been published on the safety of adding fluoride to Grand Rapids’ water supply. The people of Grand Rapids were to be unwilling test subjects.
Opponents of the fluoridation project were quickly labeled by the masterminds of Alcoa’s PR group as loonies and right-wing extremists who saw fluoridation as a communist plot. I remember these charges very well in the ’50s, having grown up during that period. Suddenly making a complete reversal of their previous stance, the USPHS and the ADA began to endorse widespread fluoridation, even before a single study of the Michigan experiment had been completed that could show fluoridation was safe, much less that it reduced cavities. But there was a compelling reason they didn’t want to wait on the results of a study, namely because initial results were showing that tooth decay rates in unfluoridated Muskegon had decreased as much as fluoridated Grand Rapids. In fact, tooth decay rates were falling in all industrialized nations well before fluoridation. Why? Because of better hygiene and nutrition.
The fluoridationists’ shenanigans were recognized as early as 1952 by Dr. A.L. Miller, a U.S. representative from Nebraska who was also Chairman of the Special Committee on Chemicals in Foods. He noted how strange it was that high officials of the USPHS would do a complete about face on the acceptability of fluoridation and within only three months of advocating extreme caution. Dr. Miller also noted that he could find no original studies by the AMA or the ADA, or any other evidence for fluoridation’s usefulness. All those associations did was refer to each other for confirmation. Representative Miller also noted the convenient connection between Oscar Ewing in his position as Federal Security Administrator, and his representation of Alcoa, which was anxious to get rid of its toxic fluoride waste.
In his book on this subject, Dr. Yiamouyiannis also points out that dissenting dentists were either censured or lost their ADA membership. Dental scientists themselves were controlled by the power of USPHS grant money: those who criticized fluoridation simply saw their grant monies dry up, a very effective tactic still used in many other areas of politicized science. The list of people involved in the fluoridation conspiracy reads like a rogues’ gallery. For example, there is John Small, the USPHS’ fluoridation expert since the 1960s. His sole job is to stem any criticism of fluoridation from any quarter, and he does his job very well. One of his major tasks is to harass, intimidate and virtually destroy anyone who dares to publicly speak or write about the dangers of fluoridation. As an’ example of his viciousness, I will share the story of Dr. Yiamouyiannis, who was once the biochemical editor of the Chemical Abstracts Service, the world’s largest chemical information center. When John Small learned that Dr. Yiamouyiannis was writing critical reviews of fluoridation, he contacted the problem doctor’s immediate superior and expressed his displeasure. In ensuing conversations with this superior, Dr. Yiamouyiannis was told that $1.1 million in federal funding was in jeopardy if he did not cease and desist his criticisms of fluoridation. The good doctor was warned several more times and finally unwilling to suppress the truth about fluoridation dangers-he was forced to resign. So much for the independence of science.
” Fluoridation is the greatest case of scientific fraud of this century. “
Robert Carlton, Ph.D., former EPA scientist, 1992
“Regarding Fluoridation, the EPA should act immediately to protect the public.
Not just on the cancer data, but on the evidence of bone fractures,
arthritis, mutagenicity and other effects. “
William Marcus, Ph.D., Senior EPA toxicologist, 1992
Unfortunately, this world is inhabited by some people who seek a profit at any cost and have no concern for public welfare and safety. The fluoride story powerfully demonstrates that we are indeed correct to be suspicious of megacorporations. We have seen how these institutions have done everything in their power to avoid civic responsibility and to manipulate the government, scientific institutions, and the medical and dental professions, all in the name of empty profit.
Most of us have been led to believe by a powerful propaganda network that fluoridation of drinking water, regular brushing with fluoride toothpaste and regular fluoride treatments are not only a good way to prevent cavities, but that the practice of fluoridation itself is very safe. Nothing could be further from the truth.
Those who promote this viewpoint have an ulterior motive and, it is not your health.
https://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.png00yarycoldhttps://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.pngyarycold2012-07-10 17:56:062012-07-10 17:56:06HISTORY OF FLUORIDE IN CAVITY PREVENTION – Dr. Russell Blaylock, Neurosurgeon
Adelaide University has had all the dental data for over five years no report has yet been published.
Despite a long history of Australian water fluoridation, there is a dearth of national data on the measured amount of adult tooth decay in Australia. Only two national surveys measuring the oral health of Australian adults have ever been done in Australia. The first adult survey was conducted in 1987-88, the second adult survey, titled the National Survey Adult Oral Health 2004-2006 (NSAOH 2004-2006) was published in March 2007, with the 8 State and Territory reports following in August 2008.
Although one of the stated aims of the 2004-2006 National Adult Oral Health Survey was to compare the amount of tooth decay in adults to their percent of lifetime exposure to fluoridated water, as at April 2012, this has still not been reported. A formal comparison of adult tooth decay, state to state, has also not been reported by the Adelaide University NSAOH report authors.
It is possible however to generally compare the tooth decay of adults in Queensland ( less than 5% of population exposed to fluoridated water before mandatory fluoridation commenced in early 2009 ), to adults in the other Australian states where the majority of adults have been exposed to water fluoridation for 30 to 40 years or more.
Within each state and territory report there is an inconspicuous section that lists DMFT values ( DMFT = Decayed teeth, plus Missing teeth due to decay, plus Filled Teeth due to decay ). DMFT values are a measure of accumulated tooth decay experience used world-wide as a reliable index of tooth decay.
The DMFT values for adults have been collated from the 8 state and territory NSAOH reports for 4 age groups and are tabulated in this document. Graphs have also been constructed of the DMFT for each age group for each state and the percentage of the population in each state with a fluoridated water supply.
Examination of the tabulated and graphed data shows that there is very little difference in tooth decay between adults who live in Queensland with little water fluoridation ( < 5% in 2007 ) to adults who live in states and territories with the majority of public water supplies fluoridated ( 70 % to 100 % of population exposed to fluoridated water )
* QUESTION – If consuming fluoridated water for up to 40 + years
has not significantly reduced or prevented tooth decay in adults
– why are Australian water supplies still being forcibly fluoridated?
Water fluoridation is forced mass medication of the population
through their own public water supplies in an attempt to
reduce tooth decay – and it has not worked.
See below:
The 8 state and territory reports of National Adult Oral Health Survey can be found at the Australian Research Centre Population Oral Health.
Only two national surveys measuring tooth decay in Australian adults have ever been published.
The first was titled the “National Oral Health Survey of Australia 1987-88: A report of the first national oral health survey of Australia ” (NOHSA 1987-88) and was published in 1993 by P. D Barnard and the Australian Dept. of Health, Housing, Local Government, and Community Services.
The second survey, titled the “National Survey Adult Oral Health 2004-2006” ( NASOH 2004-2006 )was performed as a result of a NHMRC grant obtained by dentists Prof Gary Slade and Prof John Spencer both then of Adelaide University Dental School’s ARCPOH Unit ( Australian Research Centre Population Oral Health )
On the 30th Oct 2003 the NHMRC advised Prof Gary Slade that the Minister for Health and Ageing, the Hon Tony Abbott had approved his application for a $682,500 NHMRC Project Grant to do the National Survey of Adult Oral Health project. Each of the 8 states and territories were to contribute in-kind assistance by examining the selected adults and collecting the dental data.
On the 29 July 2004 all 8 Australian State and Territory Health Ministers, along with the Federal health Minister the Hon Tony Abbott had met at the Australian Health Ministers Conference ( AHMC ) and endorsed the National Oral Health Plan 2004-2013 (NOHP 2004-2013) which gave approval and endorsement to commencing a national adult oral health survey.
The National Survey Adult Oral Health however, was already well under way when the 9 Health Ministers endorsed commencing a national adult oral health survey. Data collection had already commenced in the ACT earlier in July 2004. The NHMRC had given approval for the grant back in Oct 2003.
On the 9th Nov 2004 Prof Slade was advised by the NHMRC that the Hon Tony Abbott had approved another grant application, this time for a $2,500,000 NHMRC Capacity Building Grant in Population Health Research (CBGPHR) to extend and build on the results of the National Survey of Adult Oral Health. This NHMRC grant was titled “Oral Health Research for the Australian Population” (Chief Investigators Slade and Spencer)
A significant part of the National Oral Health Plan 2004-2013, was the endorsement of the extension of water fluoridation to all Australian communities with more than 1000 residents.
Briefing Notes provided to Federal Health Minister Tony Abbott for the AHMC 29 July 2004 meeting obtained under FOI legislation, recommended that the Federal Health Minister endorse the 2004-2013 National Oral Health Plan, but there is no mention in the Health Dept Briefing Notes that this plan was to endorse water fluoridation being extended to all communities of 1000 residents or more.
There were 5 stated aims of the National Survey Adult Oral Health Project when Prof Slade submitted his application for the NHMRC grant (Chief Investigators Prof Gary Slade and Prof John Spencer)
Aim 1: To describe prevalence and extent of dental caries, periodontal disease, tooth loss and related oral conditions. We hypothesize that all national targets for oral health by the year 2000 will have been achieved.
Aim 2: To evaluate changes in the prevalence and extent of the oral disease in the adult Australian population since the 1987/88 NOHSA. We hypothesize that compared with the 1987/88, caries experience in the Australian population will have declined for adults aged <45 years ( the “ fluoride generation” ), remained stable for people aged 45-64 years ( pre-fluoride ) and increased for people aged 65+ years.
Aim 3: To evaluate regional and socioeconomic variations in prevalence and extent of the principal oral diseases and conditions in the Australian adult population. We hypothesize that regional variations in oral diseases observed in the NOHSA will have persisted, but that socioeconomic factors explain more than half of the regional variation.
Aim 4: To describe variations in onset and progression of oral disease among “synthetic cohorts” of the Australian population that have been differentially exposed to community water fluoridation.
We hypothesize that levels of dental caries among adults who have been lifetime residents of Australian cities will be inversely proportional to the duration of community water fluoridation in those cities.**
Aim 5: To establish a prospective surveillance system that captures mortality and hospital admission data among the cohort of people examined in the 2003/04 NSAOH, thus creating a research database for future epidemiological and health services research. We hypothesize that markers of periodontal disease obtained in the 2003/04 NSAOH, will be predictors of coronary heart disease incidence and mortality within this cohort during the next decade. (NB – finalising data collection for this study still extends into the future)
NB: Aims 1 and Aim 2 were fulfilled in March 2007 when the National Survey Adult Oral Health 2004-2006 was published. The intended 2003/2004 NSAOH ended up being the 2004-2006 NSAOH.
** Profs Slade and Spencer’s Hypothesis that fluoridation reduces caries in adults inversely proportional to duration of exposure to water fluoridation appears totally incorrect – however although Adelaide University has had all the dental data for over 5 years no report has yet been published .
It is time to acknowledge that water fluoridation has neither prevented, nor reduced tooth decay in Australian adults. If the majority of the population has been exposed to fluoridated water for up to 40 years but tooth decay has not been reduced, how can continued water fluoridation be justified?
NB Tooth decay may have fallen in the younger “fluoride generation” (fluoridated toothpaste PLUS fluoridated water) (Hypothesis 2) but tooth decay has similarly decreased
in most western countries which do NOT have water fluoridation.
00yarycoldhttps://fluoridationqueensland.com/wp-content/uploads/2022/05/logo-300x77.pngyarycold2012-04-20 02:54:472012-04-20 02:54:47FLUORIDATION SURVEYS IN AUSTRALIA



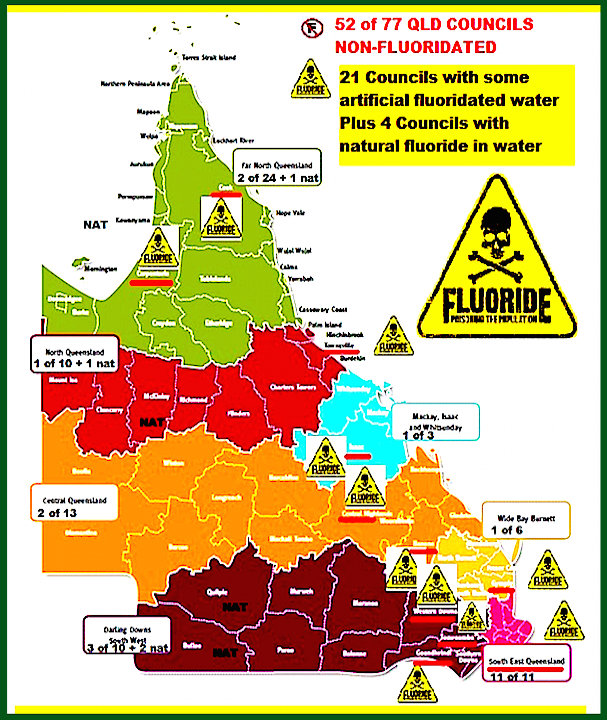







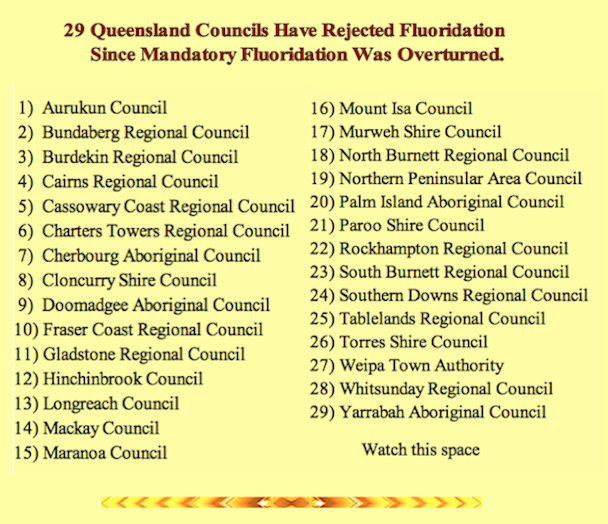
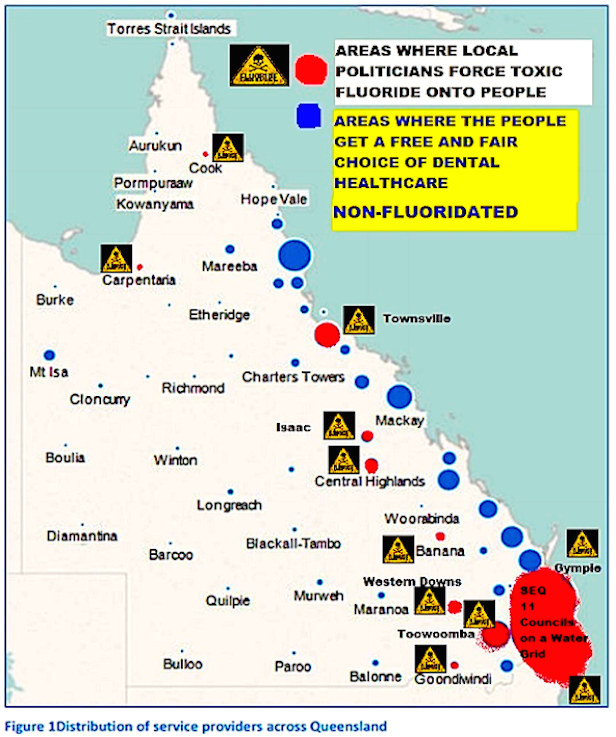




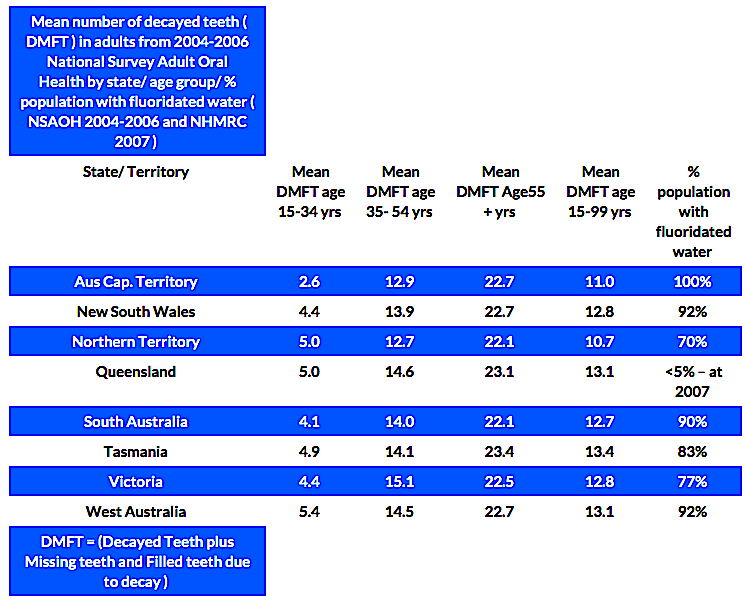
{kind=link}